Case contributions: Dr Radhiana Hassan
Clinical:
- A 14 years old girl
- Presented with sudden onset of headache and altered consciousness
- No history of fever or trauma
- Urgent non-contrast CT brain shows intraparenchymal and intraventricular hemorrhage
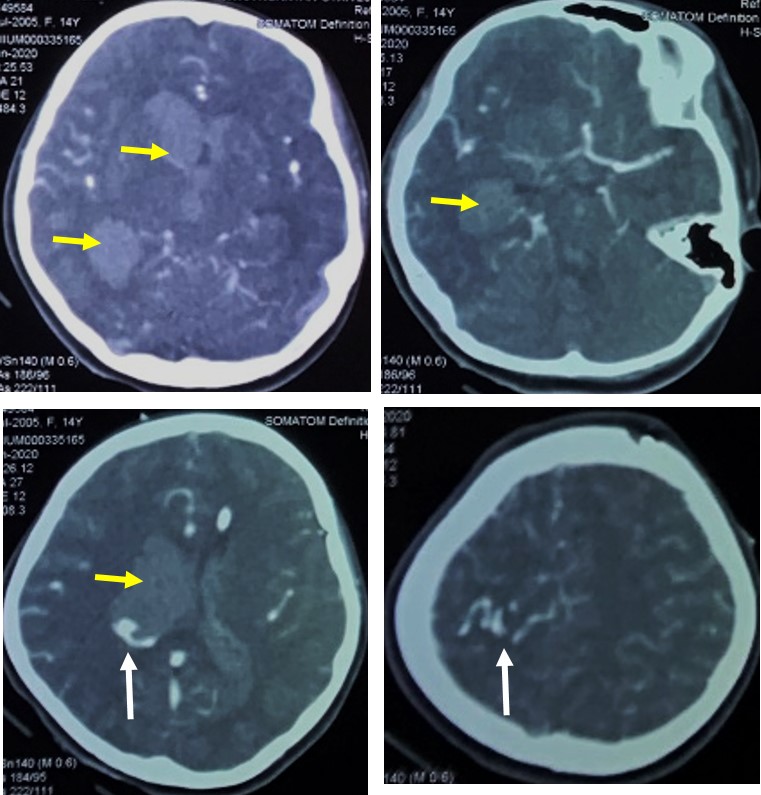
Contrast-enhanced CT scan after EVD insertion shows:
- massive intraventricular hemorrhage with hydrocephalus (yellow arrows)
- dilated vessels at right parietal region (white arrows)
- No aneurysm seen
- A dilated vessels seen with single draining vein
- No aneurysm
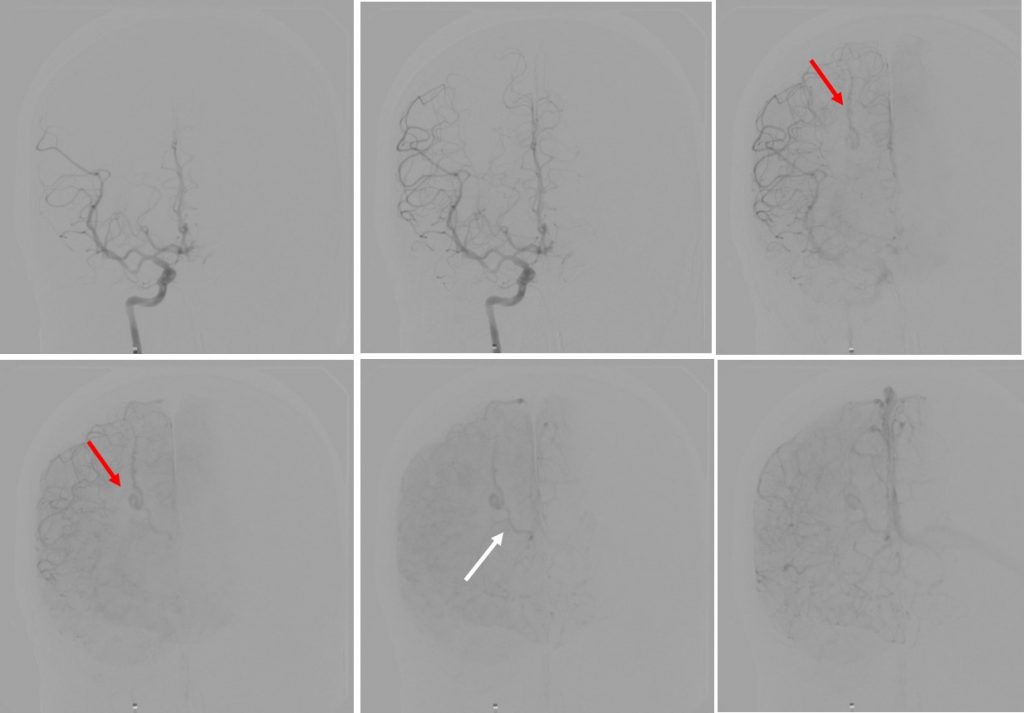
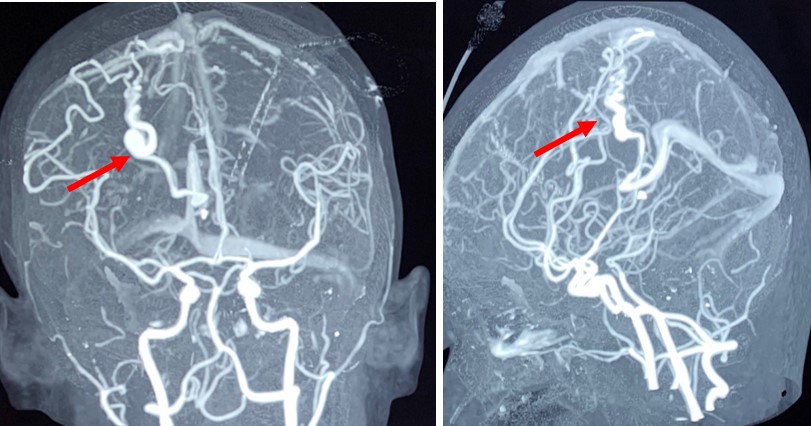
Digital subtracted angiogram shows
- A dilated artery from distal branches of callosomarginal artery on the right side
- No early draining vein seen
- No nidus, no saccular aneurysmal dilatation
- A few turn of the artery with single draining vein seen
Diagnosis: Pial arteriovenous fistula
Discussion:
- Pial AVF is a rare vascular malformations accounting for 1.6% of all intracranial vascular malformations
- It consist of a single dilated pial artery connected to an enlarged cortical draining veins
- It differs from AVM because it do not have a nidus
- It differs from dural AVF because it arise from pial artery rathet than a dural artery
- Treatment options: endovascular embolization or microsurgical resection.
- Stereotactic radiogsurgery is considered in cases difficult to reach or lesion is too small. However success is less than in AVM
Recent Comments