
Case contribution: Dr Radhiana Hassan
Clinical:
- A 45-year old lady
- Left breast lump for two weeks.
- No family history of breast cancer

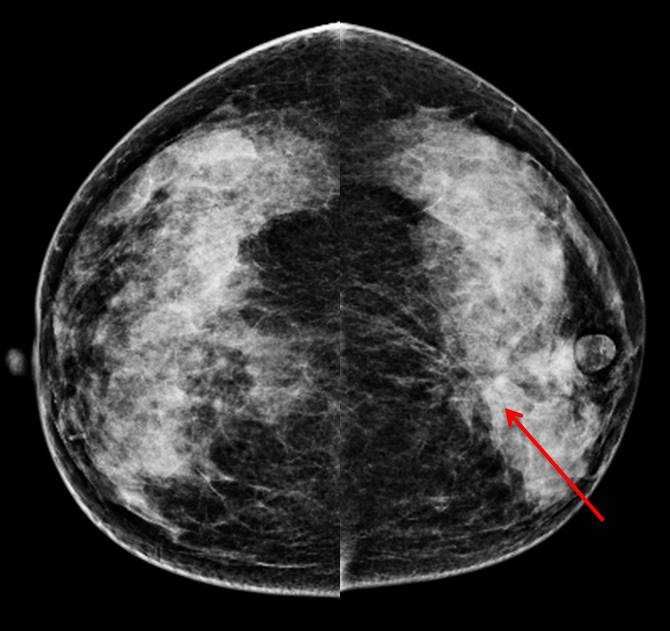
Mammogram findings:
- Bilaterally dense breasts (BIRADS C)
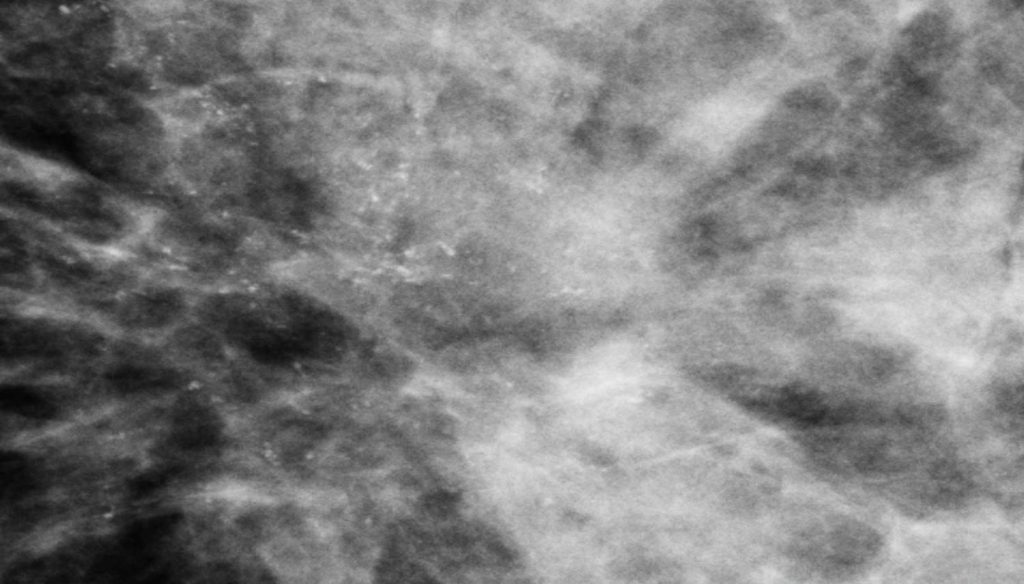
- A stromal distortion is seen at lower inner quadrant of left breast (red arrows)
- Associated clustered mircocalcifications with pleomorphism seen at the same region
- No skin thickening or nipple retraction
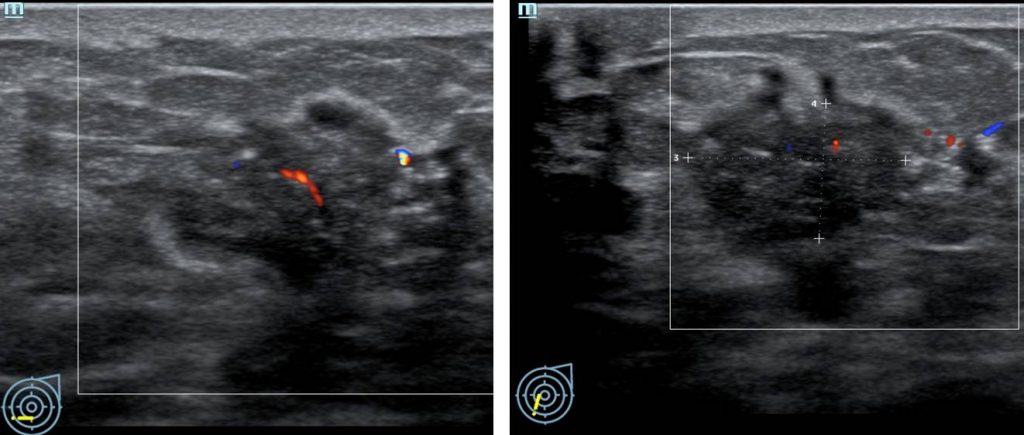
Ultrasound findings:
- A lobulated hypoechoic lesion at Lt7H measuring 23x14x12
- Multiple intralesional calcifications seen
- Associated posterior shadowing
- Presence of penetrating vessel also noted
Progress of patient:
- Tru-cut biopsy done shows invasive ductal carcinoma with 5-10% DCIS
- Mastectomy done T2N0
Diagnosis: Invasive ductal carcinoma
Discussion (clustered pleomorphic microcalcifications)
- Most breast calcifications are deposits of calcium phosphate, usually in the form of hydroxyapatite. These stain dark blue to purple on routine H and E stains. Calcium phosphate is found in a spectrum of entities that includes benign and malignant lesions.
- Calcium oxalate crystals are much less common; colorless on H and E staining; and predominantly found in benign fibrocystic epithelium, usually accompanied by apocrine epithelial metaplasia. This type of calcification is uncommon in malignant epithelium.
- Microcalcifications are calcific particles smaller than 0.5 mm.
- Grouped (or clustered) calcifications are defined as at least five calcifications within 1 cm3 of tissue, are most often of intermediate concern for malignancy of the breast.
- Most calcifications developing in breast cancer are fine pleomorphic, meaning that they vary in size, shape, and density. These calcifications are concerning for malignancy and warrant biopsy.
- Calcifications in invasive carcinoma typically are due to cell death and necrosis, which occur as the cancer outgrows its blood supply. Typically seen with invasive ductal cancer, calcifications are rarely associated with invasive lobular malignancies.
Recent Comments