
Case contribution: DR Radhiana Hassan
Clinical:
- A 15 years old girl
- History of left hand swelling for about 2 years, progressively increased in size but painless
- Claimed sustained injury during go-cart activity
- Start to have pain and restricted motion of index finger
- Radiograph was performed to rule out fracture

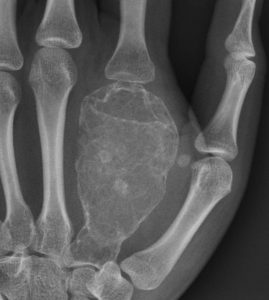
Radiographic findings:
- Marked expansion of the 2nd metacarpal bone is seen
- Extension to subarticular region but not crossing the joint
- Cortical thinning and scalloping of the endosteal surface.
- Scattered areas of increased density is seen within the bone.
- No periosteal reaction
- No obvious pathological fracture is detected.
- The other small bones of the hand appear normal.
MRI of hand:
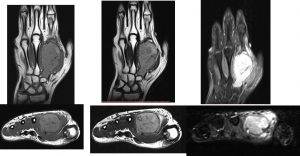
- MRI showed well-defined lesion of intermediate intensity on T1, hyperintense on T2 and TIRM.
- Presence of low signal intensity margin.
- No infiltration to surrounding muscle and soft tissue.
Differential Diagnosis:
- Enchondroma:
- Giant Cell Tumour
- Brown Tumour
Histopathology Report:
- Macroscopy: bone tumour specimen consist of greyish tissue measuring 58x32x35 mm. Cut section shows well circumscribed tumour with heterogenous greyish and brownish cut surface without necrosis. Cortical bone remains intact.
- Microscopy: Sections show a fairly circumscribed tumour composed of proliferation of osteoclast-like multinucleated giant cells in the background of numerous ovoid mononuclear cells. The giant cells have eosinophilic cytoplasm with vesicular nuclei which exhibit prominent nucleoli. There is also an occasional mitosis seen in the mononuclear stromal cells. No cortical break is noted. Skeletal muscle bundles and fibroadipose tissue is seen at the periphery of the tumour.
- Interpretation: Giant cell tumour.
Final Diagnosis: Giant cell tumour of metacarpal bone.
Discussion:
- GCT of bone also known as osteoclastomas are relatively common bone tumours.
- However, GCT of hand bones are rare. Incidence of 1.7-4%.
- A review at Mayo clinic over a period of 50 years found 14 patients with GCT of hand.
- Occurs predominantly in younger age group.
- Display more aggressive behaviour.
- Local recurrence rate post currettage and bone grafting has been reported to be as high as 90%.
- Wide resection and reconstruction with structural bone grafting has also been reported to be associated with high recurrence rate.
- Common sites: around the knee (50-65%), distal radius (10-12%), sacrum (4-9%), vertebral body (7%).
- Occurs only with a closed growth plate
- Radiographic features include: Abuts articular surface, 84-99% come within 1 cm of articular surface, Well-defined non-sclerotic margin (<5% show some sclerosis), Eccentric; if large difficult to assess, Narrow zone of transition, Overlying cortex is thinned, expanded or deficient, Periosteal reaction in 10-30% of cases, Soft tissue mass is not infrequent, with or without pathological fracture and No matrix calcification/mineralization
Progress of patient:
- Tumour excision and reconstructive surgery done
- Metatarsal bone harvested and replaced the tumour (arrow)

Recent Comments