
Clinical:
- A 54 years old male
- Presented with left sided headache, dizziness, slurred speech and right sided visual problem
- Clinical examination show right homonymous quadrantanopia
- CT Brain on the same day showed no focal lesion.
MRI findings:
- MRI done 2 weeks after initial presentation
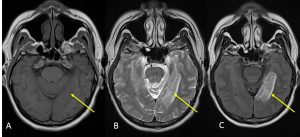
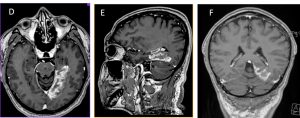
- It shows abnormal signal intensity involving the posterior aspect of the infero-medial part of left temporal and left occipital lobes.
- It is hypointense on T1WI, hyperintense on T2 and FLAIR with gyriform enhancement post contrast.
- No blooming artefact of GRE to indicate haemorrhage.
- It showed no restricted diffusion.
Diagnosis: subacute left posterior cerebral artery infarction
Discussion (PCA infarction):
- P1 extends from origin of the PCA to the posterior communicating artery, contributing to the circle of Willis.
Posterior thalamoperforating arteries branch off the P1 segment and supply blood to the midbrain and thalamus.
Cortical branches of the PCA supply the inferomedial part of the temporal lobe, occipital pole, visual cortex, and splenium of the corpus callosum. - Symptoms include contralateral homonymous haemianopia (due to occipital infarction), hemisensory loss (due to thalamic infarction) and hemi-body pain (usually burning in nature and due to thalamic infarction).
- If bilateral, often there is reduced visual-motor coordination.
- Unilateral sensory loss and hemianopia without paralysis, is generally considered diagnostic of PCA territory stroke
Recent Comments