
Clinical:
- A 55 years old lady
- Para 1, last child birth 13 years ago (2007)
- Conceived spontaneously, breast feeding for 12 months
- Initial presentation in 2008 at 43 years old with galactorrhoea
- At that time already stop breast feeding
- Remained amenorrhoea after that
- No headache, no visual impairment
- Biochemical showed increased prolactin, normal TSH
- Prolactin level normalized after treatment with dopamine agonist
MRI findings:
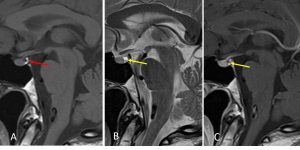
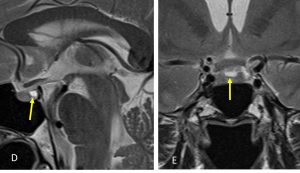
- A well defined rounded lesion in the sella, centrally located (yellow arrows)
- isointense on T1, hyperintense on T2 and not enhancing post contrast
- The lesion is located between anterior and posterior lobe of pituitary gland (red arrow)
- The lesion is very small measuring 4x3x2 mm
- No intralesional nodule seen
- No fluid levels within the lesion
- No other lesion in the brain parenchyma
Diagnosis: Rathke cleft cyst
Discussion:
- Rathke cleft cysts (RCCs) are benign, epithelium-lined intrasellar cysts believed to originate from remnants of the Rathke pouch.
- They are found in 13-33% of the general population
- Female preponderance; female to male ratio 2:1
- On imaging, it is seen as a well defined non-enhancing midline cyst within the sella arising between the anterior and intermediate lobes of the pituitary. 40% are purely intrasellar and 60% have suprasellar extension. Purely suprasellar location, although reported, is rare.
- CT scan demonstrate a hypodense lesion, non-calcified, non enhancing lesion.
- MRI appearance depends on fluid content which may be mucoid or serous. On T1WI, 50% are hypointense and 50% are hyperintense. On T2WI, 70% are hyperintense and 30% are hypointense.
- Presence of intralesional nodule is pathognomonic and seen in 75% of cases (not seen in this case).
- Differentiation with cystic pituitary adenoma: fluid fluid levels usually seen in adenoma due to hemorrhage, location non-central in pituitary adenoma and abscence of intralesional nodule
Progress of patient:
- Patient continues medical treatment
- Follow up MRI for 4 consecutive years show no change in the lesion
Acknowledgement:
- Dr Raja Nurazni, Endocrinologist
Recent Comments