
Clinical:
- A 51 years old man
- Referred to opthalmologist complaining of unable to open eyes since one month ago.
- Associated with double vision and headache
- Clinically examination shows visual acuity right and left eye 6/12, RAPD negative with total ophtalmoplegia of the left eye
- Funduscopy; clear margin and pink disc bilaterally
- Clinical diagnosis of left third nerve palsy
MRI findings:
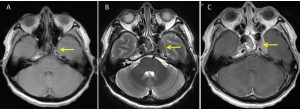
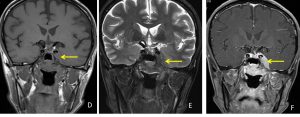
- A vividly enhancing extra axial lesion is detected within the left cavernous sinus (yellow arrows) appearing hypointense on T1 and T2.
- The lesion measures 2.7 cm (AP) x 1.0 cm (W) x 2.5 cm (CC).
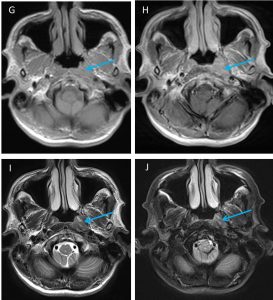
- There is abnormal fullness at left nasopharyngeal region with enhancement on post contrast (blue arrows). The change is almost similar with the cavernous sinus lesion, however no direct connection or extension is demonstrable.
- MRI features are suggestive of metastatic lesion at cavernous sinus most probably from nasopharyngeal carcinoma.
Progress of patient:
- Patient was referred to ENT team
- Additional history: Loss of weight 2 kg in 2 monthsno hearing loss, no vertigo, no neck swelling, no epistaxis, no hoarseness of voice, no stridor
- Further information, after operation 8 years ago, not sure of tissue diagnosis but patient was referred for chemoradiotherapy. He went for 2 sessions and defaulted follow up. He claimed he was well after that.
- Clinical examination showed fullness at left FOR
- Biopsy taken
HPE findings:
- Microscopy: specimen labelled as left fossa of Rosenmuller mass
- Microscopy: section shows multiple fragments of tissue partly lined by respiratory epithelium. The tissue is infiltrated by malignant cells arranged in sheets with syncytial appearance intermingled with dense lymphocytes and plasma cells. The cells display moderately pleomorphic vesicular nuclei, prominent nucleoli, and moderate amount of eosinophilic cytoplasm. Mitosis and punctuate necrosis are seen. No intercellular bridges or keratinized cells noted.
- Interpretation: consistent with nasopharyngeal carcinoma
Diagnosis: Nasopharyngeal carcinoma with metastasis to left cavernous sinus
Discussion:
- The common primary tumour for the cavernous sinus metastasis is known to be breast cancer in women and lung cancer in men.
- However, the cavernous sinus is not an uncommon location for metastases in nasopharyngeal carcinoma
- Other site of involvement in NPS include nasal cavity extension, oropharyngeal extension, parapharyngeal space extension, skull base erosion, paranasal sinus extension, hypopharyngeal extension, masticator space extension, cranial nerve palsy, intracranial invasion (such as dural invasion, brain tissue invasion and prepontine cistern invasion)
Recent Comments