
Clinical:
- A 40 years old man hit with a hammer
- Complains of headache
- No loss of consciousness
- No vomitting or blurred vision
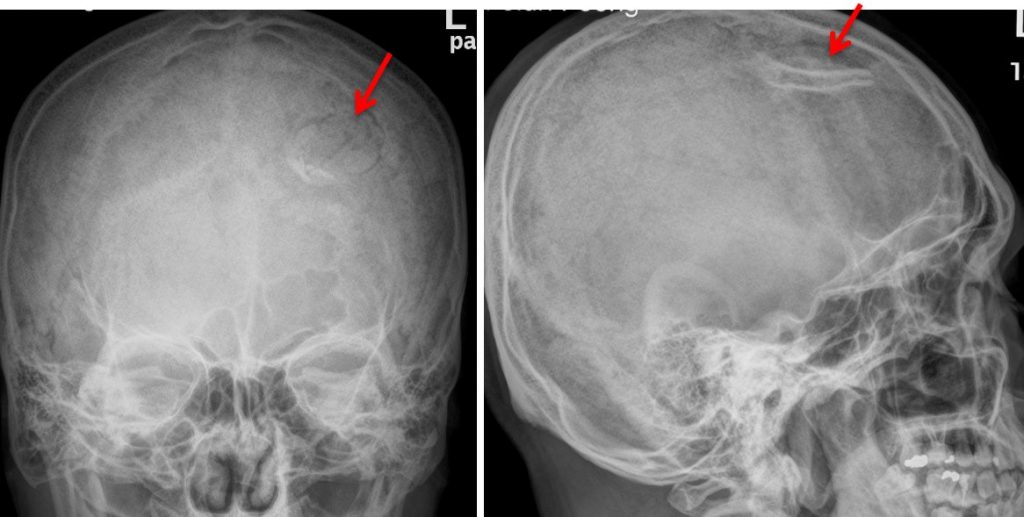
Radiographic findings:
- Abnormal lucency rounded in shape at left frontal bone
- It showed linear density on lateral projection
- No obvious soft tissue swelling is seen.
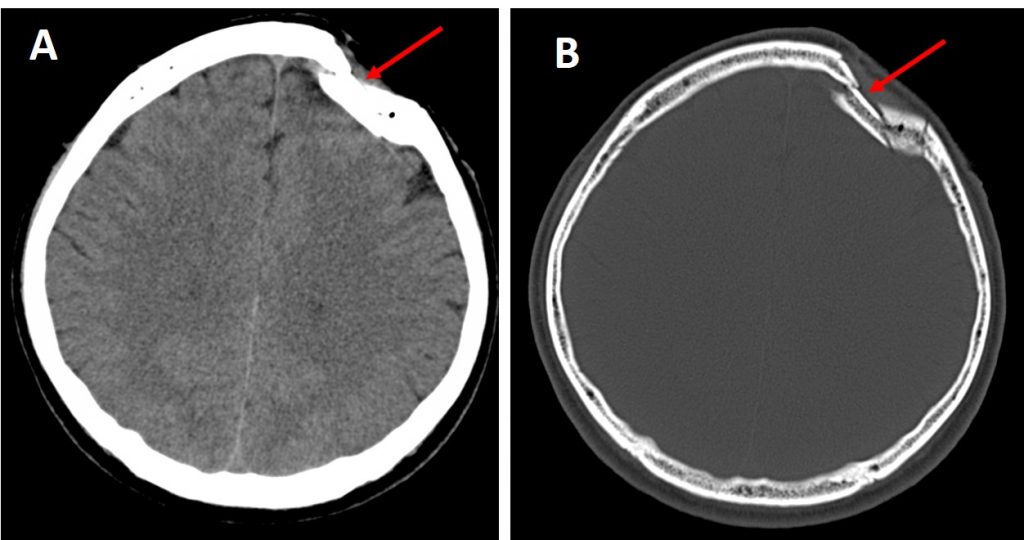
CT scan findings:
- CT scan confirmed presence of depressed fracture at left frontal bone
- There is no intracranial hemorrhage.
- No involvement of frontal sinus (image not shows)
- Minimal scalp hematoma
Discussion:
- Depressed skull fracture is fracture of the skull vault being displaced inward into the cerebral parenchyma.
- It is usually the result of a high energy impact to the skull
- These mostly (~75%) occur in the frontoparietal region.
- Open depressed skull fractures warrant antibiotic therapy and neurosurgical referral.
- Closed depressed skull fractures in which the skull fragments are not displaced more than the thickness of the skull do not require surgical intervention. However, those that are displaced greater than the skull thickness should be evaluated by a neurosurgeon because repair or elevation may be necessary to prevent further complications.
- Other depressed skull fractures that warrant neurosurgical consultation are (1) those involving the frontal sinuses, (2) those overlying the dural sinuses, (3) those involving tears of the underlying dura, and (4) more complicated depressed skull fractures with possible intraparenchymal bone fragments, even with normal neurologic findings.
- Cosmetic repair of simple depressed skull fractures may be desired by patients, although there is no evidence that such repair will change the neurologic outcome.
- Associated injuries include different types of intracranial hemorrhage, pneumocephalus and CSF leak.
Recent Comments