
Clinical:
- A 25 years old lady, health worker
- Presented with symptoms of diplopia, photophobia, headache and fever
- History of contact with TB patient
- Clinically has bilateral CN VI palsy with neck stiffness.
- Blood investigation shows elevated ESR=46mm/hr
- CSF analysis: total protein =1727mg/L, glucose=1.4 mmol/L, appearance clear, indian ink stain negative, polymorph 0, RBC=300, no growth after 48 hours
- MTB PCR +ve, HIV negative and Hepatitis B negative.
MRI findings:
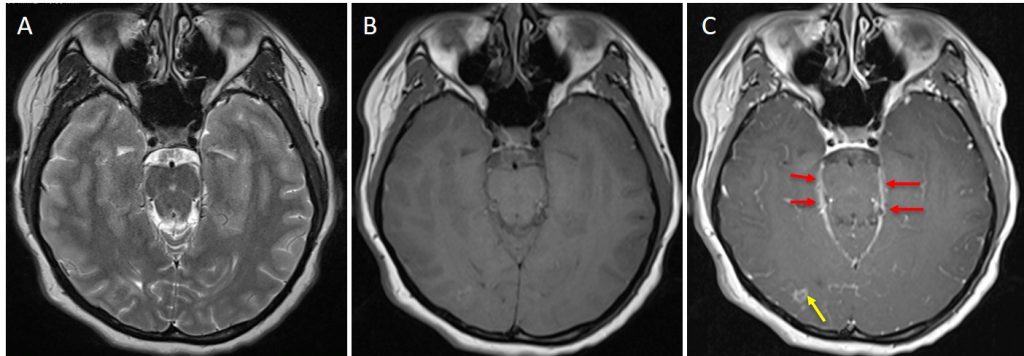
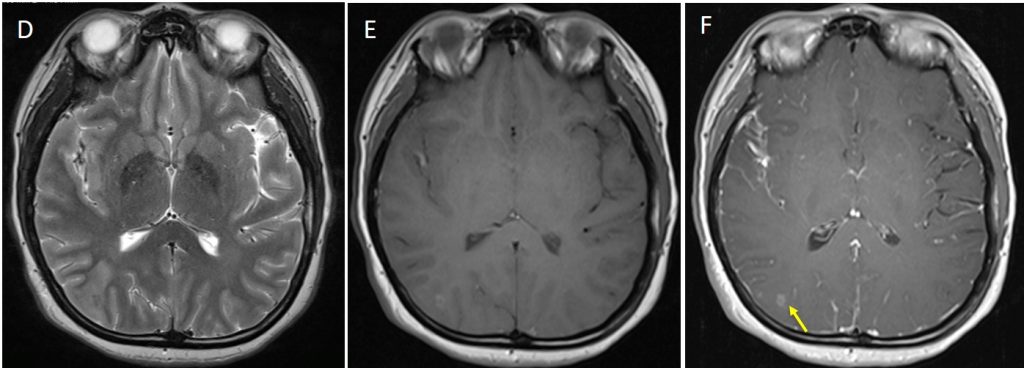
- There is diffuse leptomeningeal enhancement, but more pronounced at right sylvian fissure and basal region (red arrows).
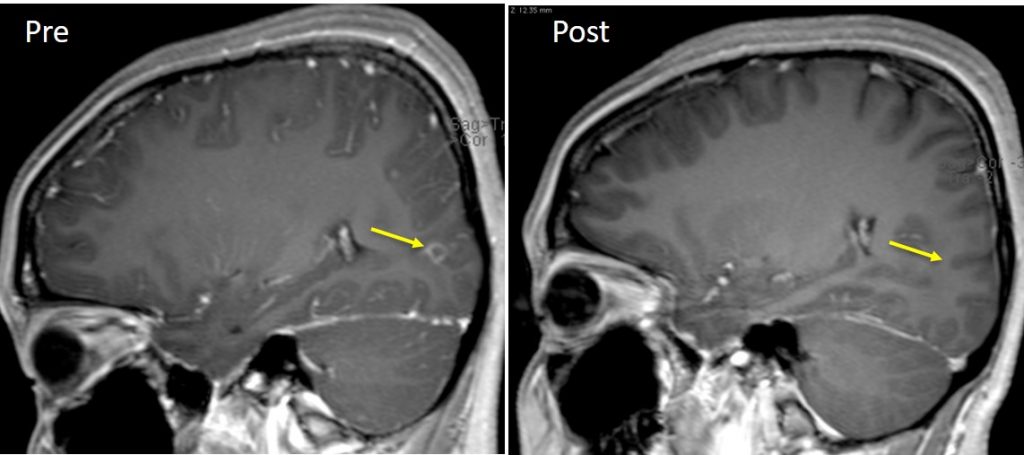
- There are small rim-enhancing lesions (yellow arrows) seen at the right occipital lobe and at the right parietal lobe which may represent tuberculomas.
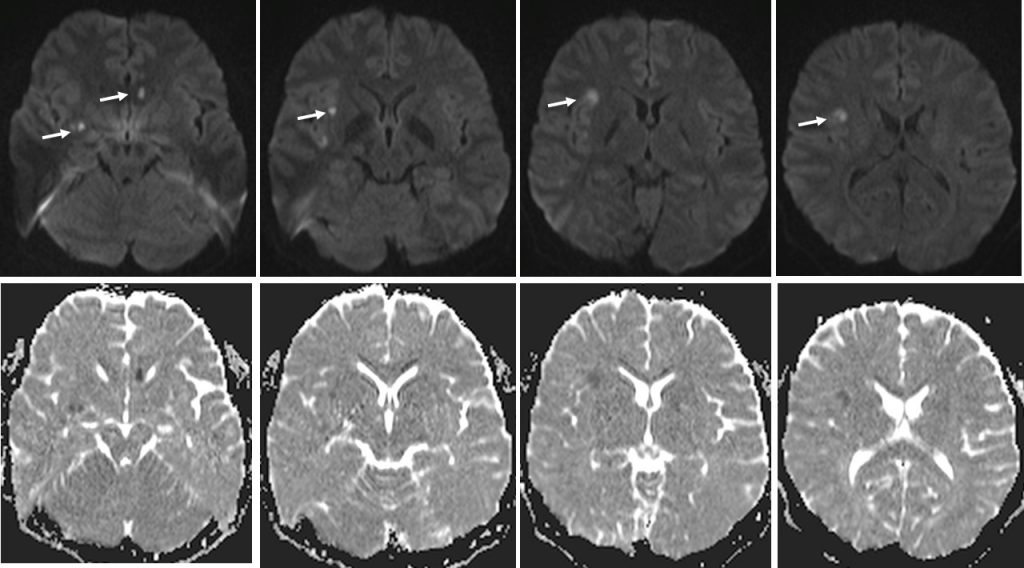
- Foci of hyperintensities on T2W are seen at the genu of left corpus callosum, right superior temporal lobe and right external capsule (white arrows). These lesions are hypointense on T1W, show restricted diffusion on DWI/ADC and do not enhance, suggestive of lacunar infarcts.
Diagnosis: CNS tuberculosis
Discussion: CNS tuberculosis
- Involvement of the CNS is seen in approximately 5% of patients with tuberculosis.
- CNS tuberculosis can manifest in many forms, including tuberculous meningitis, tuberculomas, tuberculous abscesses, tuberculous cerebritis, and miliary tuberculosis.
- In this case, meningitis and tuberculomas are seen.
- Tuberculous meningitis is the most common manifestation of CNS tuberculosis across all age groups.
- TB meningitis typical radiographic finding is abnormal meningeal enhancement, usually most pronounced in the basal cisterns. Meninges within the sulci over the cerebral convexities and in the sylvian fissures is also seen in most cases.
- Ischemic infarcts are a common complication of TB meningitis, seen in 20%–40%, mostly within the basal ganglia or internal capsule regions and resulting from vascular compression and occlusion of small perforating vessels.
- The most common CNS parenchymal lesion of tuberculosis is tuberculoma. This lesion may be solitary, multiple, or miliary and may be seen anywhere within the brain parenchyma. Tuberculomas can exist in conjunction with tuberculous meningitis, although this combination is not a consistent finding. The MR imaging findings of tuberculomas depend on whether the tuberculoma is caseating, and if so, whether the center is liquid or solid. Rim enhancement is usually seen at gadolinium-enhanced MR imaging. After treatment, tuberculomas can completely resolve; however, calcification is seen in up to one-fourth of cases and is identified most clearly at CT.
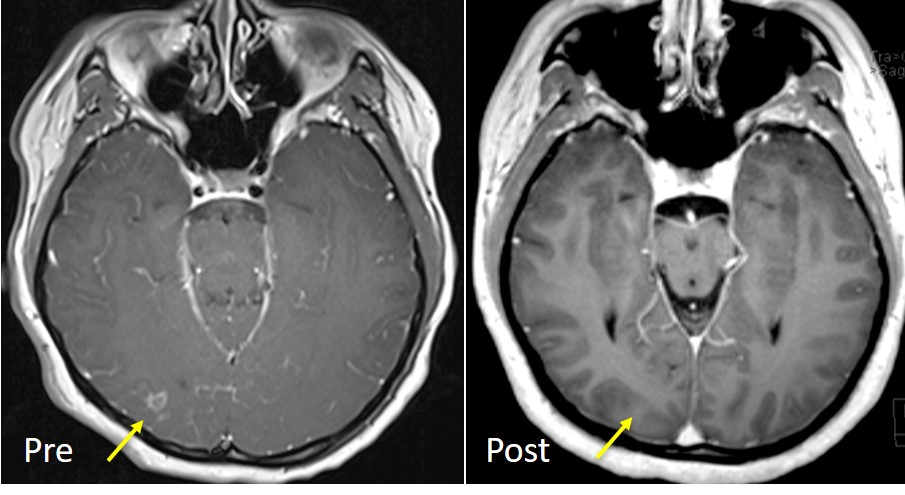
Progress of patient:
- Patient was treated with anti-tuberculous drug
- Clinically shows good response
- Repeat MRI 3 months after completion of treatment confirms good response
Recent Comments