
Case Contribution: Assoc. Prof. Dr Hilwati Hashim
Clinical:
- A 21 years old female
- Presented with 2 weeks history of right upper limb numbness and blurring of vision.
- She has had a similar episode 6 months previously which lasted for about 1 week and resolved spontaneously with no residual symptoms.
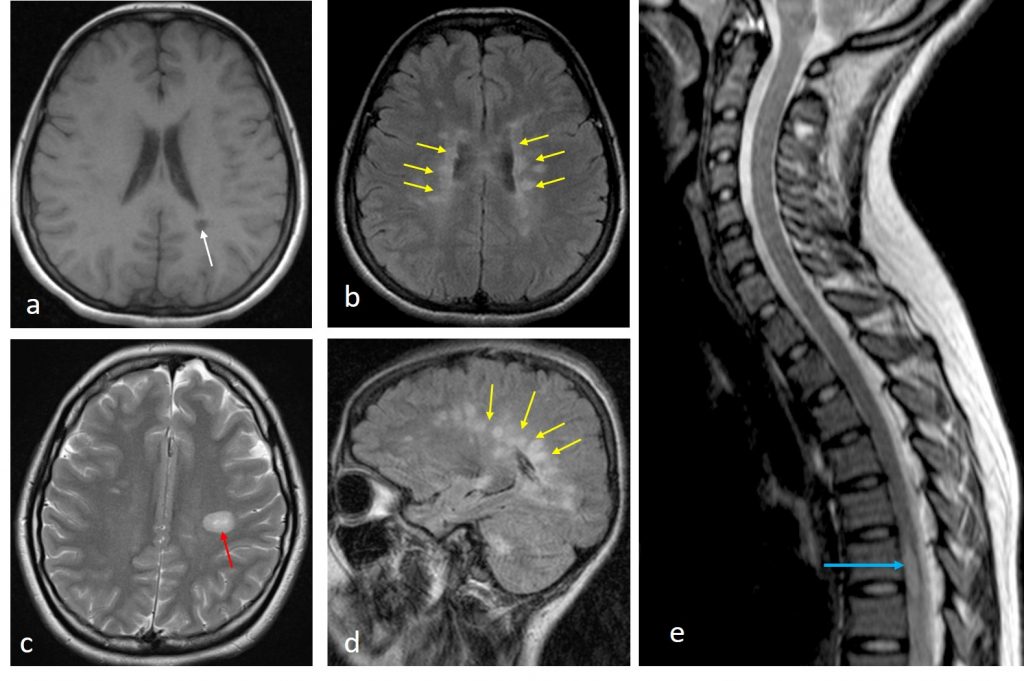
MRI findings:
- Bilateral T2/FLAIR hyperintense lesions at periventricular region which are perpendicular to the lateral ventricle (yellow arrows)
- Juxtacortical white matter at left frontal lobe (red arrow)
- A hypointense lesion on T1W at the left posterior parietal lobe “black-hole” (white arrow)
- A short segment lesion at T6 level of the spinal cord (blue arrow)
- No enhancing lesion is seen (images not shown)
Diagnosis: Multiple sclerosis.
Discussion:
- Distribution of the intracranial and spinal lesion fulfills the 2017 McDonald’s criteria for Multiple Sclerosis for Dissemination in Space.
- No enhancing lesion seen post contrast suggest that there is no active disease at the time of scan.
- Criteria for Dissemination in Time is not fulfilled in this case. If there is a baseline scan available (for example: done at the time of the previous attack), comparison can be made to look for new T2 hyperintense lesion, another criteria for Dissemination in Time.
- Lesions which are hypointense on T1WI reflects more tissue damage in term of demyelination as well as axonal loss.
- CSF analysis which demonstrates elevated IgG or oligoclonal bands is useful to support the clinical diagnosis, particularly when the clinical attacks are doubtful or MRI criteria is not fulfilled.
Recent Comments