
Case contribution: Dr Norzaini Rose Mohd Zain
Clinical:
- A 58 years old female lady was previously working as a secretary.
- She presented with rather rapid deterioration of cognitive function in the last 2 to 3 years.
- On examination, Mini Mental State Examination (MMSE) was 5/30, and her condition was associated with severe Behavioural and Psychological Symptoms of Dementia (BPSD).
- Clinical suspicion was Alzheimers Disease
MRI findings:
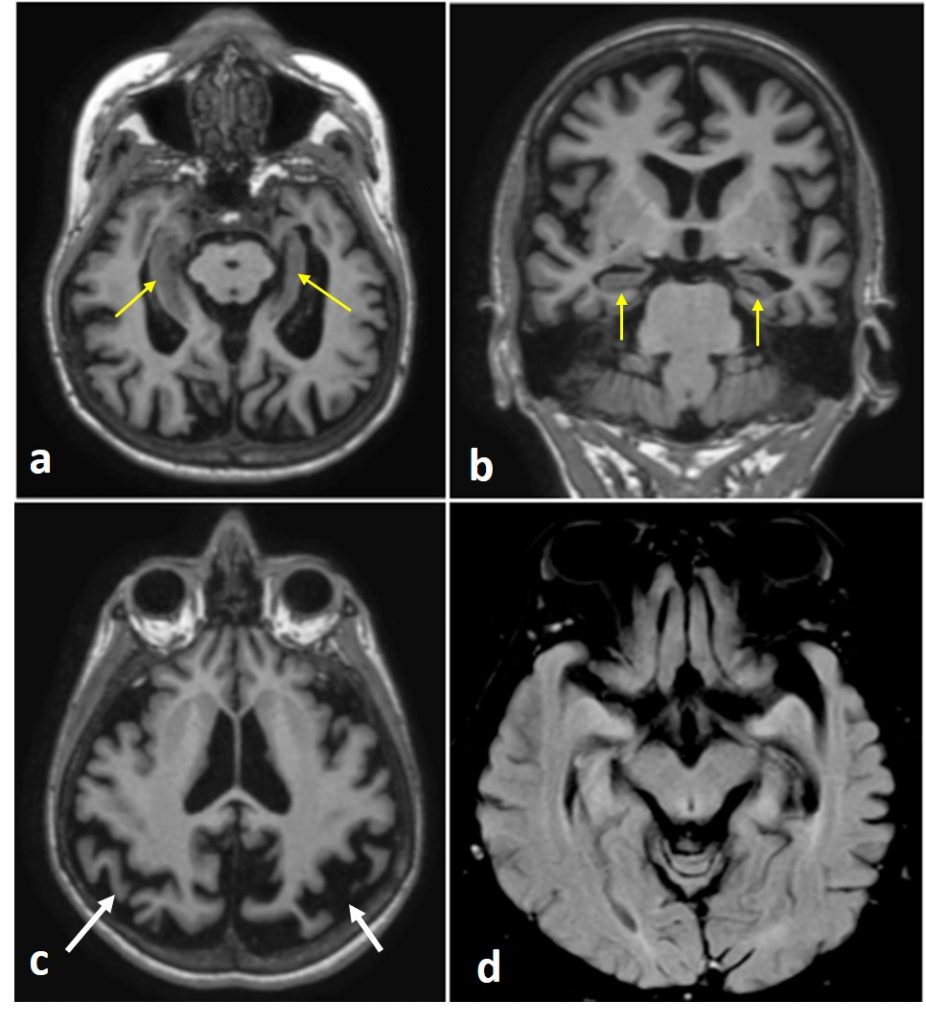
- Reformatted T1-MPRAGE images perpendicular to the hippocampus in axial (a) and coronal (b) planes demonstrate bilateral hippocampii atrophy (yellow arrows), which is worse on the left.
- In (c) there is also focal atrophy of temporo-parietal lobes (again worse on the left) in the background of global cerebral atrophy (white arrows).
- In (d) axial FLAIR image, the atrophic hippocampii show normal signal intensity.
Diagnosis: Alzheimer Disease
Discussion:
- Alzheimer disease (AD) is a progressive neurodegeneration condition that leads to cognitive decline, impaired ability to perform the activities of daily living and a range of behavioural and psychological conditions, as in this patient.
- Grossly the brain affected by AD shows generalised atrophy and shrunken gyri, widened sulci and enlarged ventricles especially the temporal horns.
- Changes are most marked in the medial temporal lobe and temporo-parietal lobes.
- The frontal lobe is commonly involved, while the occipital lobe and motor cortex are relatively spared.
- MRI reflects this pathological findings by demonstrating atrophy of the areas that are involved.
- AD has distinct clinico-pathological subtypes. The hippocampus is severely affected in 75% of cases. Relative hippocampal sparing is seen in 10% and limbic predominance accounts for 15% of AD cases.
- Typical neuropsychological profile for AD patients is memory impairment, but do note that some may present with atypical presentation such as Balint syndrome, language and frontal (executive dysfunction/behavioural) presentation
- The MRI must include a thin cut isotropic 3D images to allow image reformatting for better assessment of atrophy and corrects asymmetry in the brain that can mislead the radiological interpretation.
Recent Comments