
Clinical:
- A 23 years old lady
- Presented with gradual abdominal distension
- Not painful, no fever, no constitutional symptoms
- Normal menstrual cycle
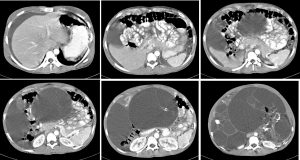
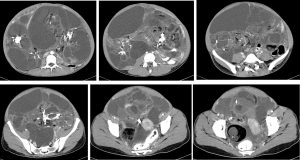
CT scan findings:
- Presence of a huge mass occupying the abdominopelvic cavity measuring 30x26x16 cm
- The lesions are multiloculated and multilobulated with heterogenous density
- Moderate enhancement of solid component is seen.
- Presence of intralesional calcification, septae and fat components are seen
- Surrounding structures are compressed and displaced
- Uterus is displaced to the left side, grossly normal in apparearance.
- Both ovaries are not identified.
- No local infiltration, no distant metastasis
- Presence of massive ascites also noted
Intra-operative findings:
- Left ovarian teratoma occupying the whole pelvic and abdominal cavity
- The mass lesion size 30x20x10 cm, multiloculated, mainly cystic with some solid areas, removed intact during surgery.
- Possible leaking preoperatively as hair are seen all over the pelvic and abdominal cavity with chronic inflammatory response.
- Right ovarian teratoma 6x4x2 cm. Cystectomy done, capsule intact
- Right and left fallopian tubes are normal
- Ascites about 800 mls probably secondary to chronic leakage of teratoma
- Uterus anteverted, 6 weeks size
- Omentum studded with chronic inflammatory granulomas, size about 1 mm diameter
- Bowel, spleen, liver and undersurface of diaphragm is normal
HPE findings:
- Macroscopy: Specimen labelled as left adnexae consists of a very huge solid cystic and lobulated mass with fallopian tube. It measures 300x300x20 mm. The cyst varies in size ranging from 12 to 230 mm in diameter. Some of the cysts are filled with clear fluid and some of them are filled with yellowish jelly-like material. The biggest cyst is filled with yellowish cheezy like material admixed with hairs. Cyst wall thickness ranging from 1 to 3 mm. Hard area is noted probably bone formation. Solid area also noted within the cyst. The fallopian tube measures 70 mm in length and 7 mm in diameter. Another specimen labelled as right ovarian cyst consist of an oval shape cystic mass measuring 70x52x47 mm. Cut section shows uniloculated cyst filled with yellowish cheesy material admixxed with hairs. Solid area is noted measuring 20x16x12 mm. The cyst wall thickness is about 1 to 2 mm. There are multiple tumour deposits on the omentum. Specimen labelled as node in POD consist of multiple pieces of tissue measuring 18 mm in aggregate diameter.
- Microscopy: section of left cystic mass shows it is composed of all layers of the 3 germ cells namely the ectoderm, endoderm and mesoderm. There is no evidence of immature elements noted. No malignancy seen. Similar changes seen of the right cystic ovarian mass. Sections from the omentum show presence of numerous foreign body granuloma surrounded by chronic inflammatory cells. There are a few hair shafts embedded within these granulomata. Two of the lymph node identified shows reactive changes. POD nodules shows deposits of numerous granulomas of variable sizes intermingled with inflammed granulation tissue, mocroabscesses and areas of fat necrosis and calcification. Small biths of hair shafts are also seen embedded within the granulomatous tissue
- Diagnosis: bilateral ovarian mature cystic teratomas and POD: foreign body granuloma.
Final diagnosis: Lipogranuloma peritonealis caused by spontaneous rupture of benign ovarian teratoma
Discussion:
- Granulomatous inflammation of the peritoneum in women may come from a variety of causes. Most of these are non‐neoplastic, such as fungal or bacterial infections, parasitic infestations, or foreign body reactions due to a previous diagnostic test or a surgical procedure.
- Rarely, the granulomatous inflammation is secondary to a neoplastic process such as the foreign body reaction elicited by contents of cystic teratomas or carcinold tumors of the ovary and uterus.
- Rupture of benign cystic teratoma into the peritoneum is a serious complication as the oily contents of the cyst may elicit a marked granulomatous reaction leading to formation of adhesions and reactive nodules called lipogranuloma peritonalis.
- It is a rare condition and can be mistaken for advanced gynecologic malignancy as initially thought in this case.
- Once the diagnosis of lipogranuloma peritonealis is established, the treatment of choice is removal of the primary tumor; however, the adhesions and granulomatous peritoneal masses are best left alone. In patients with significant residual inflammatory masses, the use of corticosteroids may improve postoperative resolution.
Recent Comments