
Clinical:
- A 53 years old lady
- Presented with progressive abdominal distension over few years
- No constitutional symptom
- No altered bowel habit
- No abnormal menses

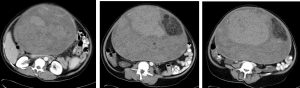
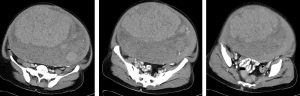
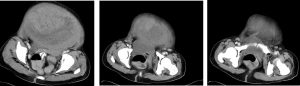
CT scan findings:
- A huge solid mass measuring 30x28x21 cm occupies abdominopelvic cavity
- The lesion displaced bowel loop peripherally
- The lesion shows well outline with heterogenous density and enhancement
- Presence of fat component noted, no calcification within or at periphery of lesion
- Unable to identify uterus and both ovaries
Intra-operative findings:
- TAHBSO, omentectomy and bilateral pelvic nodes removed
- A 34 weeks uterus, feels firm, generalised involvement, smooth surface with no obvious surface deposits
- Both ovaries and fallopian tubes are normal
- No tumour deposits
- Minimal ascitic fluid
- Multiple small pelvic nodes bilaterally
HPE findings:
- Macroscopy: specimen consists of a bisected uterus and cervix with right fallopian tubes and ovary in one half and left fallopian tube and ovary in the other half. The uterus measures 305 mm from fundus to cervix, 230 mm from cornu to cornu, 230 mm in AP diameter. Serial cut section of the uterus shows a huge tumour. Occupying the entire corpus of the uterus with nodular whitish and myxoid cut surface distorting to the uterine cavity are unable to identified the anterior and posterior endomyometrium. No necrotic areas seen. The tumour measures 250x260x220 mm. There is a well defined yellowish area seen invading the posterior tumour measures 110x90x50 mm. Both fallopian tubes and ovaries are unremarkable
- Microscopy: Sections of the uterus show an intramural lesion composed of interlacing bundles of smooth muscle fibres. Part of the lesion shows hyalinised degeneration while in another focal area there is lipomatous change. The cervix and endometrium are unremarkable. Both ovaries and fallopian tubes are normal
- Interpretation: Uterus: leiomyoma. No malignancy in the lymph nodes or omentum
Final diagnosis: Uterine lipoleiomyoma
Discussion:
- Uterine fibroids, also known as leiomyomas, are the commonest uterine neoplasms.
- They are benign tumors of smooth muscle origin, with varying amounts of fibrous connective tissue. Fibroids usually arise in the myometrium but may occasionally be found in the cervix, broad ligament or ovaries.
- Giant uterine myomas are very rare and can often create a diagnostic dilemma and therapeutic challenge owing to their size, non-specific clinical presentation and degenerations.
- Uterine lipoleiomyoma is a rare and specific type of leiomyoma with a considerable amount of adipocytes.
- Lipoleiomyoma is a benign variant of leiomyoma and is composed of mature smooth muscle cells and adipocytes with an incidence ranging from 0.03% to 0.2%.
- Fatty metamorphogenesis of the smooth muscle cells of leiomyomas is the most likely cause for the development of lipoleiomyoma. Other theories suggest that these tumors may arise due to misplaced remnants of fatty cells of the embryo, due to the extension of retroperitoneal or peritoneal fat perivascularly, due to fatty infiltration of the connective tissue, or due to the transformation of mesenchymal totipotent cell.
- Leiomyomas can be easily diagnosed on imaging in cases of typical appearances but degenerative changes or fatty content like in lipoleiomyoma may lead to change in its images and can cause difficulty and confusion in diagnosis. In this case it was initially misdiagnosed as ovarian masses based on imaging.
Recent Comments