
Clinical:
- A 48 years old man
- No known medical problem
- Complains of headache for one month
- Worsening of headache for the last few days
- No neurological deficit

MRI findings:
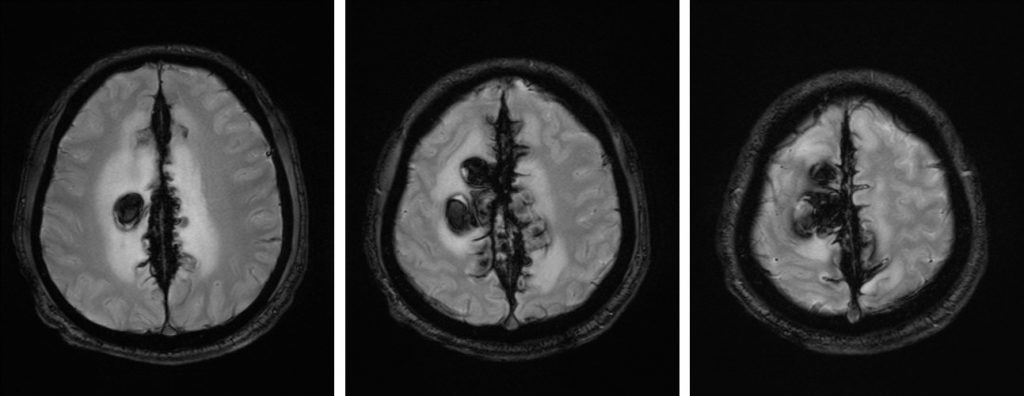
- Multiages intraparenchymal haemorrhages; mostly chronic bleed at parasagittal region of both cerebral hemispheres, more on the right side
- There is associated surrounding oedema
- Expansion of the superior sagittal sinus with heterogenous hypointensity on both T1 and T2-weighted images. There is blooming artifact noted on GRE sequence
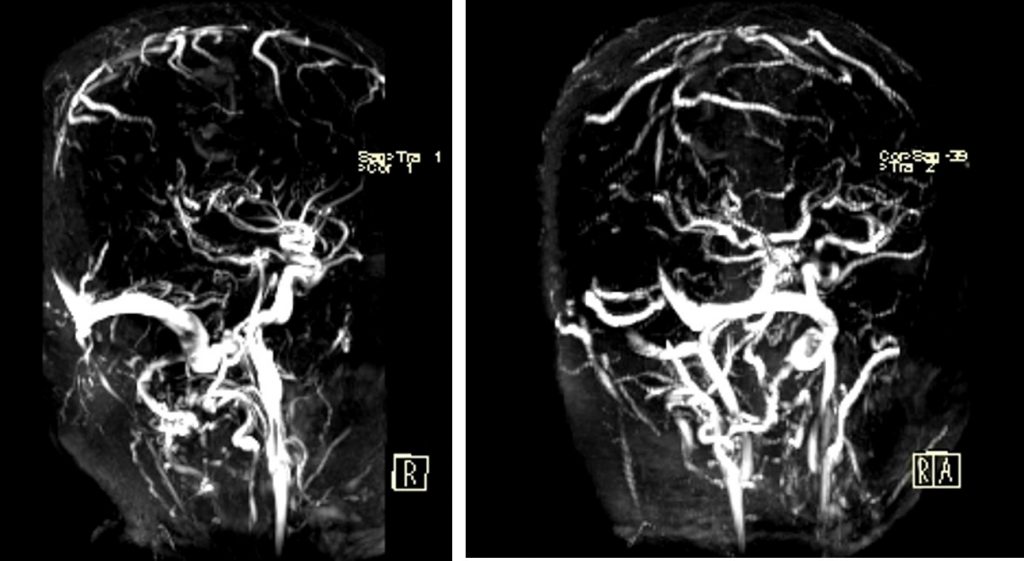
- MRV shows faint visualization of the superior sagittal sinus
Diagnosis: Superior sagittal sinus thrombrosis with intraparenchymal haemorrhage
Discussion:
- Focal brain abnormalities have been identified in as many as 57% of patients with cerebral venous thrombosis.
- Parenchymal lesions are better depicted and more commonly identified at MR imaging than at CT. Focal edema (without visible hemorrhage) is visible on CT images in approximately 8% of cases and on MR images in 25% of cases.
- In contrast with arterial ischemic states, many parenchymal abnormalities secondary to venous occlusion are reversible. Although parenchymal changes may occur in areas of the brain that are directly drained by the occluded venous sinus, in some patients the parenchymal changes may not closely correlate with the location of venous occlusion
- The signal intensity of venous thrombi on T1- and T2-weighted MR images varies according to the interval between the onset of thrombus formation and the time of imaging. The change in signal intensity is thought to be related to the paramagnetic effects of the products of hemoglobin breakdown in the thrombus (31,32).
- Chronic thrombosis with incomplete recanalization of the sinus may present a diagnostic challenge at MR imaging. As many as 15% of patients in whom sinus thrombosis is diagnosed at MR imaging may have a chronic (“15day-old) thrombus. Compared with the MR signal in normal brain parenchyma, the signal in a chronic thrombus is typically isointense or hyperintense on T2-weighted images and isointense on T1-weighted images; however, significant variability in thrombus signal intensity exists
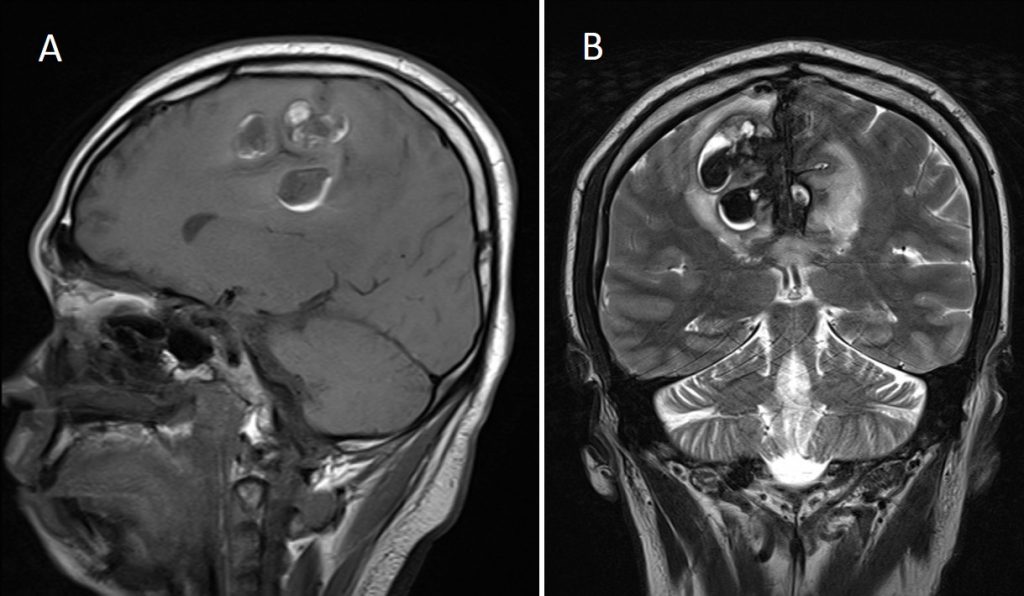
Progress of patient:
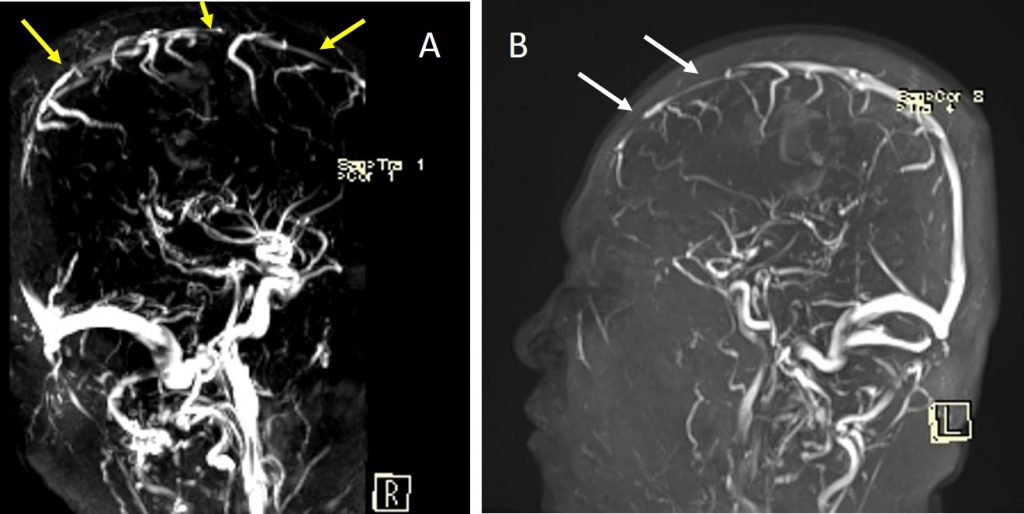
- Partial recanalization of SST post treatment
- MRI (A) before treatment and (B) 3 weeks after thrombolysis
Recent Comments