
Clinical:
- A 37 years old lady
- No known medical problem
- Para 1+1. Day 1 post SVD.
- Antenatal and intrapartum are uneventful
- Noted abdominal swelling on examination
- Further history patient claimed had pain on and off at left side of abdomen for the past 4 weeks.
- Ultrasound shows lesion suspicious of left broad ligament hematoma.
- CT scan was requested for further assessment.

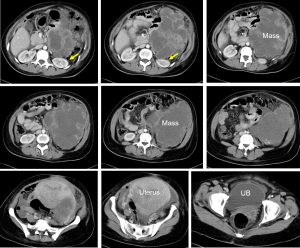
CT scan findings:
- There is a large multilobulated mass measures 17x15x16 cm in the abdominopelvic cavity lying more on the left side.
- The mass shows mixed density with cystic and solid regions. Presence of multiple septa also seen. The solid area and the septa shows enhancement post contrast.
- Peripheral displacement of bowel loops are seen. Some areas show poor plane of demarcation with bowel loops.
- Mass effect to the left kidney also noted (yellow arrows).
- The uterus is bulky consistent with recent post partum period
Intra-operative findings:
- Huge ovarian tumour arising from the left ovary measuring 20x15x15 cm, ruptured during manipulation, stucked to bowel, peritoneum and pelvic side wall.
- Left fallopian tube is normal.
- Right ovary and right fallopian tube are also normal.
- No tumour nodule at liver, spleen and under surface of diaphragm.
HPE findings:
- Macroscopy: specimen consists of a uterus with cervix, attached right ovary and fallopian tubes. The entire specimen weighs 2500 gms. Cut section of uterus shows uterine cavity filled with blood. The left ovarian tumour measures 150x120x70 mm with attached normal fallopian tube. Cut section shows a solid tumour with a greyish white cut surface. Areas of necrosis and hemorrhage are seen.
- Microscopy: The left ovarian tumour shows a large areas of necrosis and is composed of malignant cells arranges as sheets. The cells have coarse chromatin, prominent nucleolus and moderate amount of cytoplasm. There is no gland or rosette formation. Mitotic activity is brisk, 5-9/hpf. Mild lymphocytic infiltrate is seen in the fibrous septa. The omentum shows marked hemorrhage and necrosis with some viable tumour in the sections of the nodule.
Diagnosis: Dysgerminoma of left ovary with metastasis to omentum
Discussion:
- Ovarian dysgerminoma is a germ cell tumour of ovary.
- They are the most common malignant germ cell tumours of the ovary.
- These tumours occur predominantly in young women and about 10-20% of cases occur in pregnancy.
- These tumour are usually hormonally inert, however about 5% of dysgerminomas can cause elevation of serum HCG levels.
- Ultrasound shows a septated ovarian mass with varying echotexture.
- CT scan may show mass with speckled calcification. Characteristic findings include multilobulated solid massess with prominent fibrovascular septa. Post contrast can often show enhancement of the septa.
Recent Comments