
Clinical:
- A 69 years old lady
- Underlying hypertension
- Presented with back pain and bilateral limb weakness
- No history of trauma
- No constitutional symptoms

MRI findings:
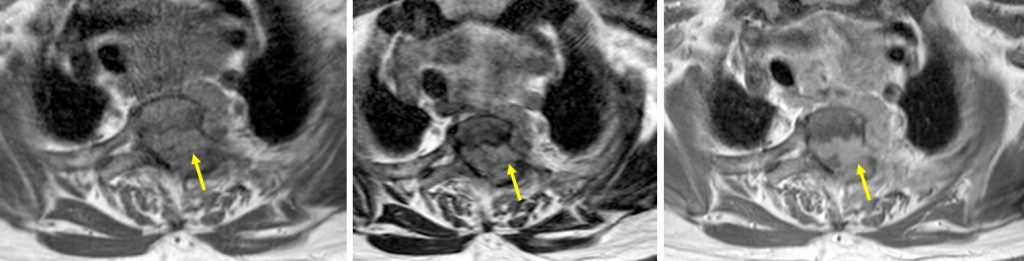
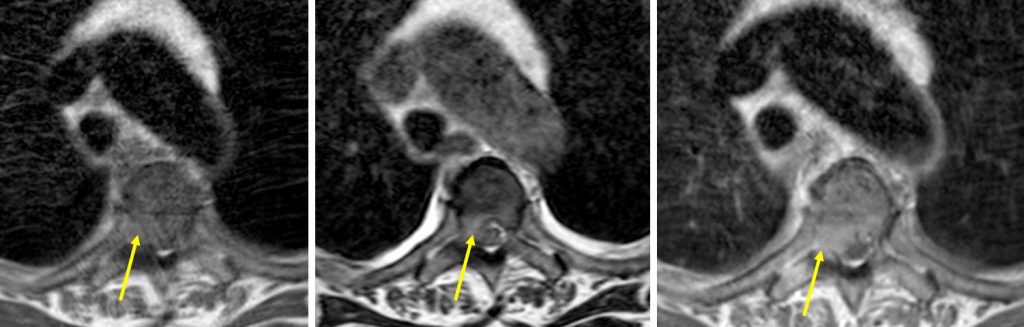
- There is reduction in vertebral body height with abnormal signal intensity seen of T5 vertebra appearing as low signal on T1, high signal on T2 and TIRM images, with non-homogeneous enhancement (white arrows).
- There is similar but more severe changes seen at T3 vertebra. Almost total collapsed of this vertebra is seen (white arrows).
- There is posterior vertebral surface convexity bulging into the spinal canal.
- Associated surrounding soft tissue mass with intraspinal extension (yellow arrows).
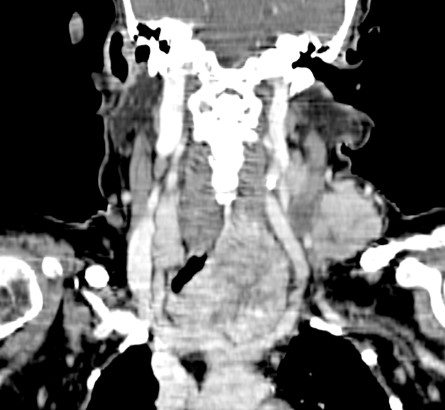
- Incidental finding of thyroid mass also noted (star-shape)
Diagnosis: Metastastic compression fractures.
Discussion:
- Vertebral compression fractures are very common, especially in the elderly.
- It is important to differentiate benign from malignant vertebral collapse because their management and outcome are substantially different.
- The spine represents the most frequent site of skeletal metastasis predominating in the thoracic and lumbar spine.
- Features supporting malignant collapse include
- Convex posterior border of the vertebral body
- Abnormal signal intensity of the pedicle
- Epidural mass
- Focal paraspinal mass
- involvement of the posterior half of the vertebral body
- contrast enhancement and
- multi-segmental involvement of vertebrae.
Progress of patient:
- Further work-up confirms diagnosis of thyroid carcinoma with multiple skeletal metastasis
Recent Comments