
Case contribution: Dr Raja Rizal Azman
Clinical:
- A 1-year old girl presents with seizures resistant to antiepileptic medication and developmental delay.
- The patient was a term baby with no complications during delivery.
- The patient began having infantile spasms at 4 weeks of age. At the age of 4 months the patient began to develop tonic contractures in extension of both upper limbs with preserved consciousness.
- Currently the patient suffers 3-4 episodes daily lasting 1-3 minutes.
MRI findings:
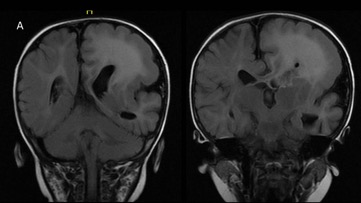
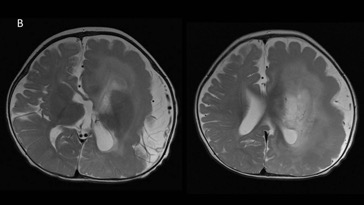
- FLAIR (figure A) and T2-weighted images (figure B) shows asymmetric enlargement of the left cerebral hemisphere with diffuse thickening of the left cerebral gyri and shallow sulci.
- There is diffuse white matter hyperintensity of the left cerebral hemisphere with minimal contralateral shift of the anterior and posterior falx cerebri.
- The body and frontal horn of the left lateral ventricle are small.
- No areas of calcification. The brainstem and cerebellum are normal.
Diagnosis: Hemimegaencephaly
Discussion:
- Hemimegaencephaly is caused by unilateral cerebral hamartomatous overgrowth.
- Disordered neuronal migration results in areas of extensive pachygyria, polymicrogyria and grey matter heterotopia.
- The condition is divided into isolated, syndromic and total hemimegaencephaly.
- The syndromic type is associated with Klippel-Trenaunay syndrome, Proteus syndrome, tuberous sclerosis and Neurofibromatosis type 1.
- Total hemimegaencephaly is the most uncommon type with involvement of the brainstem and cerebellum.
- The presentation is usually of macrocephaly with intractable seizure disorder in early infancy and severe developmental delay. The imaging findings are an asymmetrically enlarged cerebral hemisphere with thickened gyri and shallow sulci representing areas of abnormal gyration.
- There may be areas of calcification within the white and grey matter.
- The white matter is usually diffusely hyperintense on FLAIR, due to abnormal myelination.
- Anatomic or functional hemispherectomy remains a good therapeutic choice for seizure control in patients with hemimegaencephaly in spite of the high associated rate of mortality and morbidity.
Recent Comments