
Case contribution: Dr Radhiana Hassan
Clinical:
- A 42 years old man
- No known medical illness
- Presented with low back pain
- Associated with mild physical exertion
MRI findings:
- Normal alignment of the lumbar vertebrae. The vertebral body heights are normal.
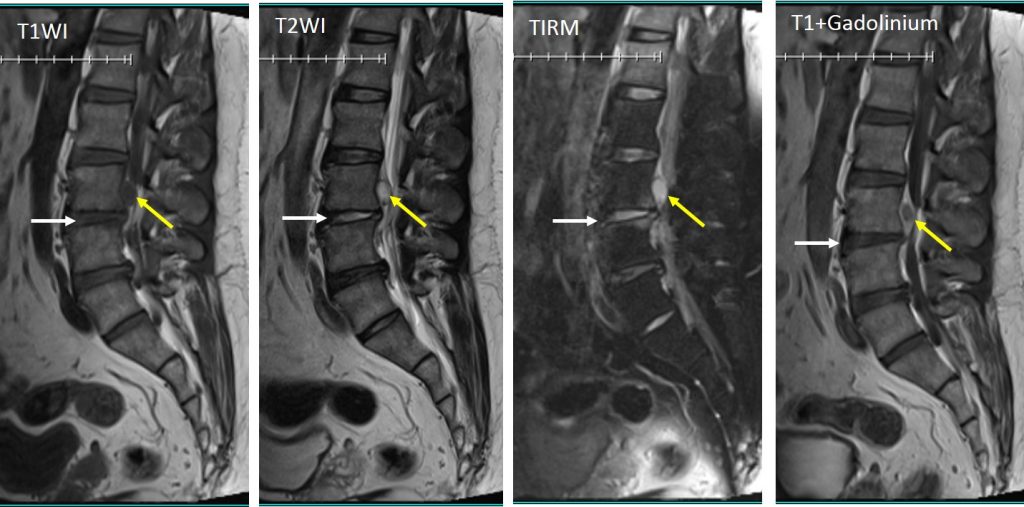
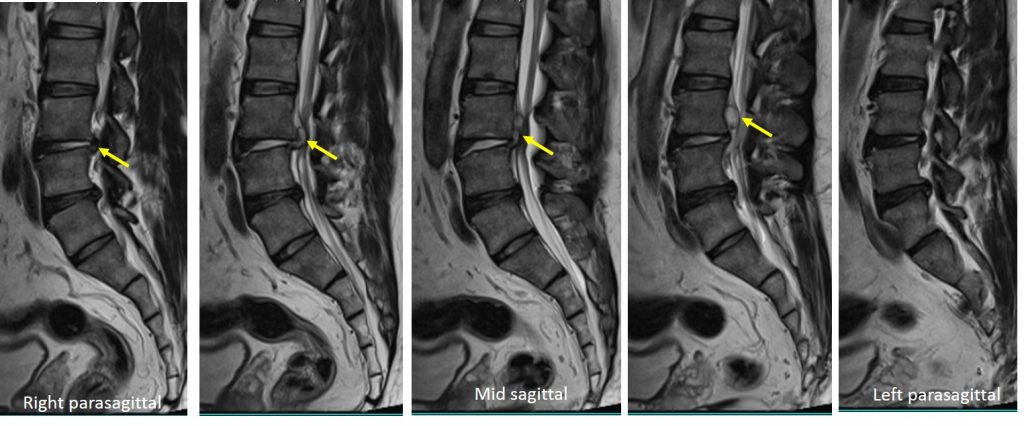
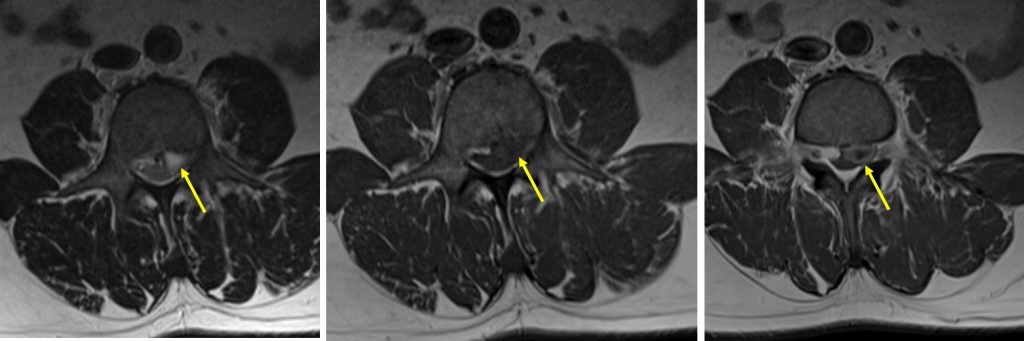
- Posterior to the L3 vertebral body, there is an oval-shaped lesion (yellow arrows) which is hypointense on T1, hyperintense on T2 and not suppressed on fat suppression sequence. This lesion showed peripheral rim enhancement on post contrast image.
- The signal intensity is similar with the L3/L4 disc in all sequences. The disc at this level is also reduced in height (white arrows).
- This lesion measured about 13x11mm in size.
- It is located more towards left side of the spinal canal.
- Lesion posterior to L3 vertebra is suggestive of sequestered disc.
Diagnosis: Disc sequestration (proven intra-operatively)
Discussion:
- Disc sequestration corresponds to extruded disc material that has no continuity with the parent disc and is displaced away from the site of extrusion.
- It is also called free disc fragment or migrated disc.
- The disc fragment can compress the spinal nerve root, causing pain and symptoms similar to herniated discs.
- Migrated disc fragments usually appear hyperintense in 80% of cases on T2-weighted images, and hypointense on T1-weighted images, as compared with the disc origin.
- Rim enhancement after gadolinium injection is usually shown around the extruded fragment and is related to the presence of inflammatory response and neovascularization as in this case.
- Hematomas, abscesses and synovial cysts followed by neoplasms like schwannoma and mengioma are the specific lesions most frequently misdiagnosis with posterior sequestrated disc herniation.
Recent Comments