
Case contribution: Dr Radhiana Hassan
Clinical:
- A 67 years old man presented with left loin pain
- No hematuria
- No constitutional symptoms
- US shows a mass lesion at left renal
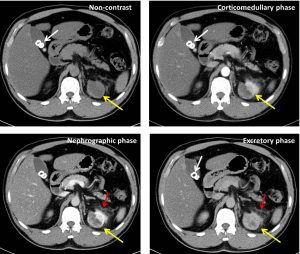
CT scan findings:
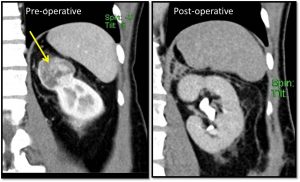
- There is an irregular lobulated soft tissue lesion seen at the upper pole of left kidney (yellow arrows) measuring about 3.9 (AP) x 4.0(W) x 3.8cm (CC). Marked peripheral heterogenous enhancement seen at corticomedullary and nephrographic phase. The delayed phase shows gradual enhancement of central lesion. Streakiness of the adjacent left pararenal fat is noted (red arrows).
- No filling defect seen in the IVC to suggest thrombosis.
- No renal calculus or hydronephrosis seen bilaterally.
- No lesion in the right kidney.
- Incidental finding of cholelithiasis (white arrow)
Diagnosis: Renal oncocytoma (HPE proven)
Discussion:
- Renal oncocytoma is a benign tumour, accounting about 3-7% of all renal tumours.
- This lesion is difficult to be distinguish from renal cell cell carcinoma (epidemiology, presentation, imaging and histology can be very similar).
- Typically present in the 6th to 7th decade of life.
- Peak incidence at 55 years.
- There is 2:1 male predilection
- A biopsy is usually not helpful in distinguishing oncocytoma from a renal cell carcinoma as both may have oncocytic elements.
- The imaging appearance of oncocytomas is difficult to be distinguish from renal cell carcinoma.
- The wide spectrum of imaging findings in renal oncocytomas are due to the differences in tumour cellularity and its hemorrhagic/cystic changes.
- It appears as a sharply demarcated lesions of various sizes but often large at presentation.
- Presence of central stellate scar is characteristic of oncocytomas but is only seen in a third of cases. RCC may also demonstrate a central scar.
- The only reliable feature is evidence of metastasis of aggressive local infiltration in which the diagnosis of renal cell carcinoma can be safely made.
- Small lesion shows homogenous enhancement whereas larger lesion shows heterogenous enhancement.
- High cellular components demonstrate avid arterial enhancement and subsequent washout.
- Low cellular components demonstrate gradual subsequent enhancement owing to abundant stroma.
- Cystic and hemorrhagic changes may account for lesion heterogeneity in the delayed phase.
- Perinephric fat stranding may be seen due to oedema
- Calcification may be present. Necrosis is usually absent.
- Renal vein thrombosis may be present but tumour thrombus is absent.
- Multifocal oncocytomas and oncocytomas coexisting with renal cell carcinoma are not rare.
- Renal oncocytomas may demonstrate interval growth.
Progress of patient:
- Partial nephrectomy done in another hospital
- HPE came back as oncocytoma
- Repeat US and CT scan 3 years later shows no recurrence
Reference:
- Imaging spectum of renal oncocytomas: a pictorial review with pathologic correlation. Ishigami K et al. Insights Imaging 2015 Feb; 6(1): 53-64
- Renal oncocytoma. Bickle I and D’Souza D. Radiopedia at https://radiopaedia.org/articles/renal-oncocytoma
Recent Comments