
Case contribution: Dr Radhiana Hassan
Clinical:
- A 65 years old man
- Underlying DM, HPT
- Also had bilateral staghorn calculi. PCNL done for the left renal calculus.
- Presented with fever, dysuria and suprapubic pain for 3 days.
- Associated with chills and rigor. No hematuria.
- Noted low BP and started on medication
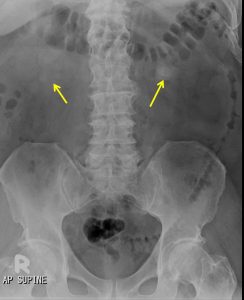
Radiographic findings:
- Faint opacities seen overlying both renal shadows (yellow arrows)
- The renal outline is partially obscured by bowel gas and fecal material
- Obliteration of both psoas outline
- Degenerative change of the spine
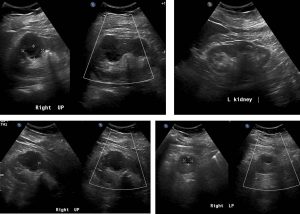
Ultrasound findings:
- There is a fairly well-defined multiseptated lesion at upper pole of right kidney measuring about 4.0 cm x 4.7 cm (AP x W). No intralesional debris, calcification or increased vascularity seen within.
- Another small well-defined anechoic lesion is seen at lower pole of right kidney which measures about 1.5 cm x 1.5 cm (AP x W). No intralesional septation or increased in vascularity seen.
- There is echogenic calculus with posterior shadowing seen occupying the right renal pelvis likely represents staghorn calculus.
- No focal lesion within the left kidney. No hydronephrosis or hydroureter seen bilaterally.
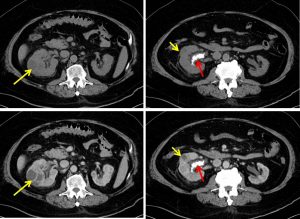
CT scan findings:
- There are several rim-enhancing hypodense lesions seen in both kidneys.
- The largest of these lesions is seen in the right kidney interpolar region measuring 3.5 x 3.9 x 3.9 cm (AP x W x CC). This particular lesion can be seen to contain multiple septations. This lesion causes a focal bulge on the renal outline.
- No calcification or air pocket is seen within all of these lesions.
- Minimal fat streakiness is observed in both perinephric fat, more apparent on the right side. Both Gerota and Zuckerkandl fascias are intact bilaterally.
- Multiple calculi are again seen occupying the right renal pelvis, forming a staghorn calculi.
Diagnosis: Renal abscesses.
Progress of patient:
- Patient had an episode of atrial flutter secondary to sepsis during admission
- Percutaneous US guided drainage done.
- About 20mls of thick haemopurulent fluid was aspirated and sent for laboratory investigations (no growth).
- Post aspiration shows significant reduction in abscess size.
- Patient recovered well.
Discussion:
- Renal abscess is a collection of infective fluid in the kidney.
- It is usually develop as a sequelae of acute pyelopnephritis
- It can affect all ages with no sex predilection
- Predisposing factors include: DM, renal calculi or ureteral obstuction
- On ultrasound, a renal abscess appears as a well-defined hypoechoic area within the cortex. It demonstrate internal echoes within. Associated diffusely hypoechoic kidney due to acute pyelonephritis has been reported. Perinephric collection may also be seen.
- CT scan is the most accurate modality for diagnosis and follow-up of renal abscesses.
- An abscess appears as a well-defined mass of low attenuation with a thick, irregular wall or pseudo capsule, which is better visualized on contrast enhanced scans.
- Gas within a low attenuation/cystic mass strongly suggests abscess formation.
- Associated fascial and septal thickening is seen with obliteration of perinephric fat.
Recent Comments