 cell carcinoma")
Case contribution: Dr Radhiana Hassan
Clinical:
- A 38 years old man
- Non-smoker
- No known medical illness
- Presented with painless hematuria for about one year
- No fever, no constitutional symptoms
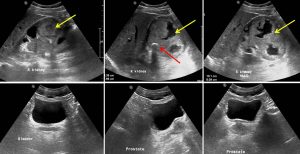
Ultrasound findings:
- Right kidney is enlarged measuring 13 cm in size.
- There is a large soft tissue mass at the lower pole of the right kidney (yellow arrows) measuring 9.3 x 8.0 cm in size with irregular cystic areas within it.
- There are specs of calcification seen within the mass (red arrow).
- No increase in vascularity is seen within it. Unable to trace IVC or renal vein.
- Left kidney is normal. Urinary bladder is also normal.
- Prostate is normal in size.
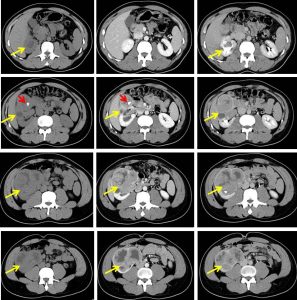
CT scan findings:
- The right kidney is enlarged with the bipolar length measures about 13.9 cm.
- A large, heterogeneous minimally enhancing mass (yellow arrows) is seen predominantly occupying the anterior aspect of interpolar region and the lower pole of the right kidney, measuring about 8.1 cm (AP) x 9.6 cm (W) x 10.0 cm (CC).
- Two foci of calcifications (red arrow) are seen within the superior and inferior aspect of the mass. No fat component is observed.
- The mass appears to be located within the calyces and causes thinning of the renal cortex which is still enhancing on post contrast images.
- It extends medially into the renal pelvis and proximal right ureter.
- Moderate pelvicalyceal dilatation is observed at the upper pole of the right kidney with no contrast excretion observed into the right ureter.
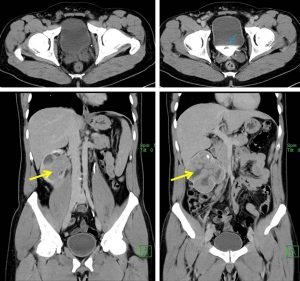
- Perinephric fat stranding with prominent vessels are noted surrounding the inferior part of the mass.
- A small filling defect (blue arrow) is seen within the urinary bladder. No wall thickening is seen.
- No filling defect is seen within the right renal vein and IVC.
- No infiltration to surrounding structures.
HPE findings:
- Macroscopy: specimen labelled as right kidney consists of nephrectomy specimen comprises a kidney measuring 120x80x80 mm, attached ureter measuring 205 mm (length) and 12 mm (diameter). Cut sections of the kidney show a huge irregular tumour mainly involving the renal pelvis up to the ureteropelvic junction and extending into the renal calyces measuring about 84x80x64 mm. The tumour appears to invade the renal parenchyma, however no renal capsular breach is seen. The tumour is friable with papillary projections seen. It has greyish cut surface with extensive areas of necrosis and hemorrhage. The perinephric fat is 1-8mm and appears uninvolved by the tumour. The Gerota fascia is free from tumour. The tumour is 180 mm from ureteric margin, 5 mm from renal artery margin, 5 mm from renal vein margin and 4 mm from the Gerota fascia.
- Microscopy: sections show an irregular tumour arising from the renal pelvis and composed of malignant urothelial cells arranged in solid sheets, papillary and nesting patterns. The tumour has invaded beyond the muscularis into the the renal parenchyma. The tumour pushes near the renal capsule, however no capsular breach or perinephric invasion is seen. The malignant cells display moderate nuclear pleomorphism with irregular hyperchromatic nuclei, conspicuous nucleoli and moderate to abundant clear pale to eosinophilic cytoplasm. Mitosis is easily seen. Occasional bizarre cells are observed. Area of necrosis are noted. No other divergant differentiation seen. The stroma shows desmoplasia with moderate to dense lymphocytic and plasmacytic infiltrates. No obvious lymphovascular or perineural invasion seen. The adjacent urothelium shows dysplasia. The renal sinuses are spared from tumour involvement. The surrounding renal parenchyma is atrophic. Sections of the uninvolved ureter show benign urothelium with some intraepithelial lymphocytes. The stroma shows mild to moderate lymphocytes and plasma cells infiltrates with lymphoid aggregates noted. NO dysplasia or carcinoma in sity of the ureter. The distal margin is clear from malignancy. The renal artery and veins margins are clear from tumour involvement. No lymph node or gland are seen.
- Interpretation: high grade urothelial carcinoma of the renal pelvis TNM stage pT3. The tumour has invaded the renal parenchyma. No lymphovascular or perineural invasion seen. The distal ureteric margin, renal artery and renal vein margins are clear from malignant cells
Diagnosis: Transitional cell carcinoma (urinary tract)
Progress of patient:
- URS: right renal pelvic tumour seen, no biopsy taken
- Cystoscopy examination: sediment/cloudy urine, bleeding from the right ureteric orifice, no bladder tumour noted
- Open nephroureterectomy done. Intraoperative findings: renal mass measuring about 12×8 cm, retroperitoneal organ adjacent to the renal mass intact, not infiltrated by the tumour
- 4 months after operation, CE under LA done for urethral strictute. Dilatation done. No bladder growth seen.
- CE at 8 months post op noted a urinary bladder growth at 11-12 o0clock. HPE low grade non-invasive papillary urothelial carcinoma. Intravesical mitomycin given
Discussion:
- Transitional cell carcinoma (TCC) is also called urothelial cell carcinoma (UCC)
- It is the most common primary malignancy of the urinary tract and may be found along its entire length, from the renal pelvis to the bladder.
- It accounts for 85-90% of all uroepithelial tumours
- Transitional cell carcinoma is typically a tumor of older patients, with the average age of presentation being 65
- There is a strong male predilection (M:F = 4:1)
- Bladder is 30-50 times more often the site of tumour than ureter or renal pelvis.
- Synchronous (simultaneous) transitional cell carcinomas are common
- Metachronous (sequential) transitional cell carcinomas in upper tract
- Imaging findings:
- IVU: enlarged and hydronephrotic kidney, dilated calyces with filling defect within
- US: discrete hypoechoic mass within the renal sinus
- CT scan: dilated collecting system and intraluminal mass
- Angiography: hypovascular mass, vessel enhancement and stain
Recent Comments