
Case contribution: Dr Radhiana Hassan
Clinical:
- A 51 years old man
- No known medical illness
- Active smoker
- Presented with sudden onset of right iliac fossa pain
- Associated with fever and vomiting
- No bowel habit change
- Similar symptoms twice few months before, spontaneously resolved with self medication
- Clinically stable, abdomen soft, localized guarding at right iliac fossa, no ascites
- Blood investigation Hb:12.8, TWBC:11.7

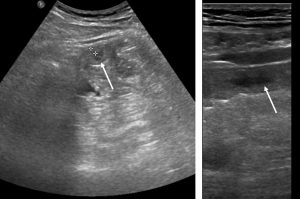
Ultrasound findings:
- There is a focal thickening of bowel wall at right iliac fossa region, may represent the terminal ileum
- No obvious dilatation of the bowel seen.
- The appendix is not visualized. However, no evidence of collection seen within the appendicular region.
- No obvious abnormality of the caecum identified.
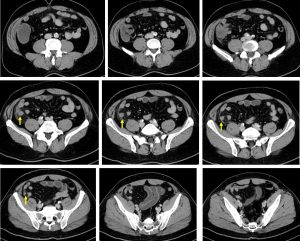
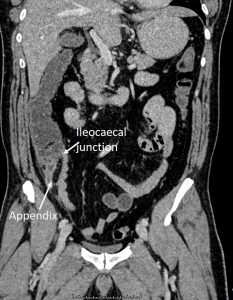
CT scan findings:
- The appendix appears heterogenous and dilated measuring about 1.3 cm.
- The appendix wall is thickened associated with periappendiceal fat stranding.
- No hyperdense structure intraluminal to suggest appendicolith.
- Bowel loops are not dilated.
- No ascites.
Progress of patient:
- Laparoscopic converted to laparotomy done on the same day after CT scan
- Intra-operative findings: pus at right paracolic gutter, clumping of bowel covering appendix, no perforation, base ishealthy
- Appendicectomy done.
- HPE confirmed appendicitis.
Diagnosis: Acute appendicitis
- Acute appendicitis is a very common condition and is a major cause of abdominal surgery in young patients.
- CT is the most sensitive modality to detect appendicitis but its use should be limited because of the radiation dose required especially in young patients
- Ultrasound should be employed as first-line where possible.
- Ultrasound is performed with graded compression using the linear probe over the site of maximal tenderness, with gradually increasing pressure to displace normal overlying bowel gas.
- Ultrasound findings include distended appendix, surrounding (echogenic) inflamed fat, thickening (edema) and then later, thinning (pre-rupture) of the appendix wall. Collections (hypoechoic areas) around the appendix can also be seen.
- CT is highly sensitive (94-98%) and specific (up to 97%) for the diagnosis of acute appendicitis. CT scan findings are almost similar what is seen on ultrasound.
Acknowledgement:
- Dr Siti Kamariah Che Mohamed.
Recent Comments