
Case contribution: Dr. Radhiana Hassan
Clinical:
- A 64 years old man
- Underlying DM and gouty arthritis not on proper treatment or medication
- Presented with hematuria for one month
- Worsening past 3 days
- Associated with blood clots and mucus
- Denies passing sandy urine or pus
- Associated with occasional fever

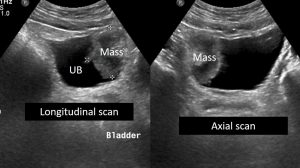
Ultrasound findings:
- There is no lesion in both kidneys. No hydronephrosis bilaterally (images not shown).
- Urinary bladder shows a papillary soft tissue mass measuring 4.1 x 3.3 cm size, arising from its right wall and projecting within urinary bladder cavity.
- Prostate is not enlarged with no focal lesion within.
- No ascites.
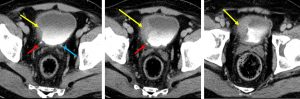
CT scan findings:
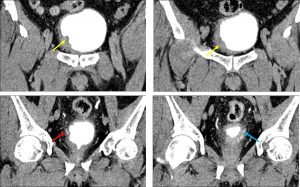
- There is a lobulated fungating and enhancing soft tissue mass projecting into the lumen of the urinary bladder. It is seen arising from the lateral part of right urinary bladder wall extending to the right vesicoureteric junction (yellow arrows).
- The maximal thickness is measuring about 2.3cm.
- Associated bladder wall thickening is seen adjacent to the mass, which extend to the bladder neck.
- The mass is however not causing obstruction to the right ureteric orifice (red arrows). The left ureter is also normal (blue arrows).
- Prostate gland is normal in size, measures about 3.2 AP x 3.1 W x 3.5cm CC.
- Clear demarcation is seen in between the bladder mass and seminal vesicle, prostate as well as adjacent bowel loops.
- No significant pelvic or para-aortic nodes enlargement seen.
HPE findings:
- Macroscopy: specimen labelled as bladder tumour and tumour bed.
- Microscopy: sections show fragments of malignant urothelial tumour arranged as fused papillary configuration infiltrating the stroma. The polarity of the urothelium is loss. The individual tumour cells are pleomorphic, having vesicular nuclei and exhibit prominent nucleoli. The cytoplasm is abundant and dense in areas. The mitosis is brisk including the abnormal mitotic figure. Area of necrosis is present. Muscular invasion seen.
- Impression: Infiltrating urothelial carcinoma, high grade with muscular invasion seen
Diagnosis: Urothelial carcinoma of the bladder
Discussion:
- Urinary bladder cancer ranked as the fourth most common malignancy.
- Bladder cancer typically occurs in men aged 50–70 years and is related to smoking or occupational exposure to carcinogens.
- The most common subtype is urothelial carcinoma which accounts for 90% of cases. Squamous cell carcinoma accounts for 2%–15%, adenocarcinoma represents less than 2%. Mesenchymal tumors represent the remaining 5% of bladder tumors, with the most common types being rhabdomyosarcoma, typically seen in children, and leiomyosarcoma, a disease of adults. Rarer mesenchymal tumors include paraganglioma, lymphoma, leiomyoma, and solitary fibrous tumor. Small cell carcinoma is a rare type of bladder tumour.
- Urothelial cell carcinoma is also known as transitional cell carcinoma is the most common urinary tract cancer.
- On CT scan it appear as either focal regions of thickening of the bladder wall, or as masses protruding into the bladder lumen, or in advanced cases, extending into adjacent tissues. The masses are of soft-tissue attenuation and may be encrusted with small calcifications.
- Most urothelial tumours are located at bladder base (80%).
- About 60% of tumours are single and measures less than 2.5 cm at time of diagnosis.
- Urothelial carcinoma has a propensity to be multicentric with synchronous and metachronous bladder and upper tract tumors. Multicentric bladder tumors occur in up to 30%–40% of cases. Upper tract tumors occur in 2.6%–4.5% of bladder tumor cases and are seen most frequently when multiple bladder lesions are present.
Progress of patient:
- Patient was referred to oncoligist, defaulted follow up and refused further treatment
- Diagnosed NSTEMI while admitted but not started on ACS treatment due to persistent hematuria and anemia
- Patient died 3 months after diagnosis due to major cardiac event secondary to massive hematuria
References:
- Neoplasms of the urinary bladde: Radiologic-Pathologic correlation. RadioGraphic 2006 at https://doi.org/10.1148/rg.262055172
- Transitional cell carcinoma (urinary bladder) at https://radiopaedia.org/articles/transitional-cell-carcinoma-urinary-bladder
Recent Comments