
Case contribution: Dr Radhiana Hassan
Clinical:
- A 28 years old man
- Previously healthy, Alleged mva
- Admitted for pelvic bone fractures
- Noted poor urine output after 2 days post trauma
CT scan findings:
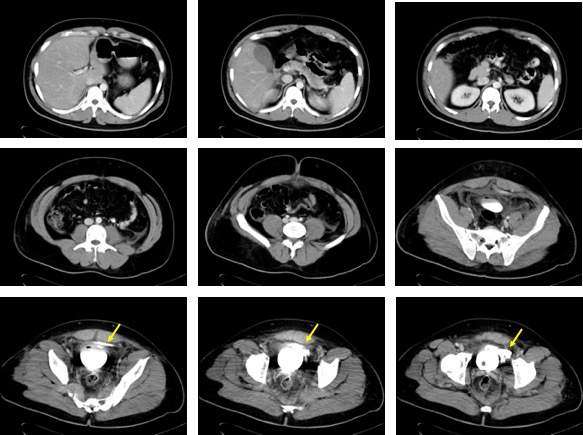
- No injury of liver, spleen, pancreas and both kidneys are seen.
- Contrast extravasation from urinary bladder (yellow arrows)
- Irregular pooling of extravasated contrast material at perivesicle region
- No outlining of bowel loops or intraperitoneal extension of contrast
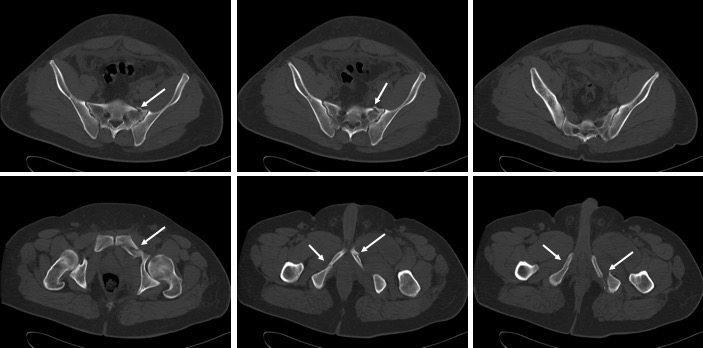
- Multiple fractures (white arrows) involving the left sacral alar and both pubic rami.
- No widening of sacroiliac joint and symphysis pubis
Diagnosis: Extraperitoneal urinary bladder injury
Discussion:
- Bladder injury is categorized anatomically as being either intraperitoneal (15–30%), extraperitoneal (40–60%), or mixed (10–25%).
- Blunt external trauma to the bladder usually occurs due to rapid acceleration-deceleration forces stressing the fascial attachments of the bladder to the pelvis and horizontal tearing near fascial connections.
- Extraperitoneal rupture is the most common type of urinary bladder injury, accounting for about 85% of cases.
- Extraperitoneal injury is usually associated with the posterior bladder wall and fibrous attachments, including the pubovesical ligament, puboprostatic fascia in men, superior fascia, and inferior fascia.
- Approximately 12% of trauma patients have a pelvic ring injury. Additionally, injury to intra-abdominal or pelvic organs occurs in 3–6% of patients with pelvic fractures and 15% with severe pelvic fractures
- Cystography reveals a variable path of extravasated contrast material.
Recent Comments