
Case contribution: Dr Radhiana Hassan
Clinical:
- A 19 years old
- Under follow up for arachnoid cyst Grade 2 at left temporal region
- Presented with left temporal headache for 3 days, unable to sleep, pain score 8/10
- Associated with vomiting.
- No blurring of vision, no fever, no slurred speech, no limb weakness
- Clinical examination was unremarkable
CT scan findings:
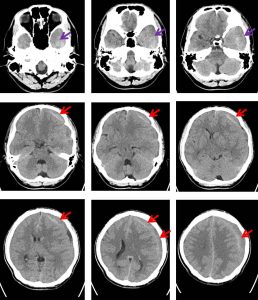
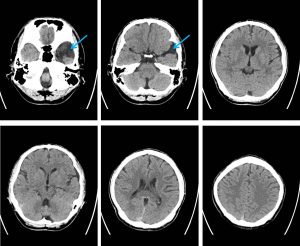
- There is a large left subdural collection (HU: 40-50) involving the left fronto-temporo-parietal region (red arrows). Its maximum thickness is about 2.5 cm at the left vertex.
- No layering within the collection and it appears hypo- to isodense to white matter.
- Generalised effacement of the sulci in the involved region is observed.
- Similar density seen at left temporal region (purple arrows). Previously reported left arachnoid cyst is not well demonstrated in this study
- There is midline shift about 1.1 cm towards the right side with subfalcine herniation.
- Body, frontal and occipital horns of left lateral ventricle as well as 3rd ventricle are compressed.
Diagnosis: Subacute subdural hemorrhage in the left cerebral hemisphere with possible intracystic hemorrhage into left subarachnoid cyst.
Discussion:
- Arachnoid cysts are benign developmental cavities of the subarachnoid space, containing a fluid close in composition to that of CSF and lined by a membrane of true arachnoid cells.
- It is one of the most frequently lesions constitute 1% of intracranial space-occupying lesions and are most commonly found in middle cranial fossa.
- Most arachnoid cysts are asymptomatic, and they often go clinically unnoticed.
- Symptoms are usually related to an increased intracranial pressure, size, or location of the cysts.
- Although most arachnoid cysts remain stable in a life period reported changes and complications include complete disappearance, intracystic hemorrhage, enlargement, and rupture causing subdural hemorrhage that may occur spontaneously over their natural course or after exertion, physical activity, or a traumatic insult.
- Spontaneous intracystic hemorrhage with or without associated subdural hemorrhage as well as arachnoid cysts with no intracystic hemorrhage but with associated SDHs or chronic subdural hygromas have also been reported
- Even though the risk of hemorrhage in patients with arachnoid cyst is very low, the presence of AC is a known risk factor for SDH.
- Fortunately, the clinical outcome of patients who present with hemorrhage associated with arachnoid cyst is generally favorable with early recognition and prompt surgical treatment.
Progress of patient:
- Left burr hole and drainage of left frontoremporoparietal subdural hemorrhage done
- Noted motor oil appearance
- EVD drain inserted
Recent Comments