
Case contribution: Dr Radhiana Hassan
Clinical:
- A 69 years old man
- Presented with hematuria, fresh blood with clots
- Usually painless, had pain after passing out blood clot on current episode
- Also complaint of difficulty to pass urine
- Lethargy for the past 2 weeks
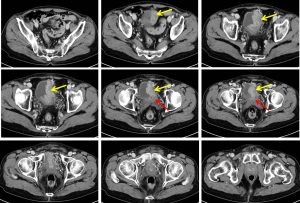

CT scan findings:
- A lobulated enhancing intravesical mass arising from the lateral wall of the bladder (yellow arrows) is seen measures approximately 7.2 x 3.1 x 4.5 cm (AP x W x CC).
- The mass now occupies half the urinary bladder.
- The mass also extend into the prostate gland and the seminal vesicle (red arrows).
- Anterior laterally it extends through the bladder wall into the adjacent fat.
- The anterior abdominal wall is not involved.
- Dilated tortuous vessels are seen surrounding the bladder.
- The rectum and sigmoid colon are preserved.
- Subcentimetre pelvic lymph nodes
HPE findings:
- Macroscopy: specimen labelled as bladder tumour, consist of multiple pieces of brownish
- Microscopy: sections show fragments of tissue composed of malignant cells arranged in solid sheets and infiltrating into the surrounding desmoplastic stroma. The malignant cells exhibit moderate pleomorphic, hyperchromatic to vesicular nuclei with prominent nucleoli. Mitotic figures are abundant. Areas of necrosis are also present. No muscular tissue included.
- Interpretation: infiltrating urothelial carcinoma, high grade.
Intraoperative findings:
- TURBT done.
- Bladder tumour at dome and left lateral wall
- Bladder tumour at the dome not completely resected to avoid perforation
- Left meatus stricture dilated up to size 28Fr
- Iatrogenic inferior wall urethral mucosa stripping
Discussion:
- Majority of bladder cancers are seen in males older than 60 years old.
- Risk factors include smoking, chronic infection and exposure to amines
- Ninety-five percent of bladder tumours are transitional cell carcinomas with the rest are mix of squamous cell carcinoma, adenosquamous cell carcinoma and rare sarcoma.
- Transitional cell carcinomas are also called urothelial cell carcinomas.
- Seventy percent of bladder cancers are superficial in origin.
- TO determine whether a potentially curative cystectomy should be attempted, the surgeon needs to know whether the disease is confined to the bladder wall (Stage II) or extends to perivesical fat (Stage III).
- Tumours may be polypoid or sessile and often extend to involve a large area of the bladder wall including the ureterovesical junction. TCC is often multifocal and evaluation of entire urinary tract is essential.
- Number and size of pelvic and retroperitoneal node should also be assessed.
Recent Comments