
Case contribution: Dr Radhiana Hassan
Clinical:
- A 78 years old with underlying HPT and DM
- Presented with being less responsiveness for 2 weeks, appears confuse and lethargic
- Noted to have facial asymmetry on the day of presentation.
- GCS E3V5M6, pupils 3mm reactive bilaterally, power left UL 3/5, LL 4/5 and both right UL and LL 5/5. To look for CVA.
- TWC 11.6, CRP 1.86.
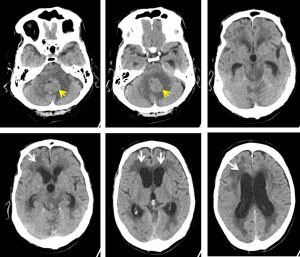
CT scan findings:
- There is a mass iso to slightlyly hyperdense to white matter seen at the interhemispheric region of the cerebellum which measures about 2.2 cm x 3.0 cm x 2.4 cm (AP x W x CC)-yellow arrows.
- Associated surrounding vasogenic oedema is observed. No midline shift.
- Bilateral lateral ventricles including both temporal horns and also third ventricles are dilated with surrounding transependymal seepage of CSF in keeping with acute hydrocephalus (white arrows).
- No acute intracranial hemorrhage is detected.
- The rest of grey and white matter junction differentiation is preserved.
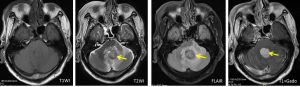
MRI findings:
- There is a well-defined mass (yellow arrows) which is seen adjacent to the 4th ventricle (predominantly from its left part).
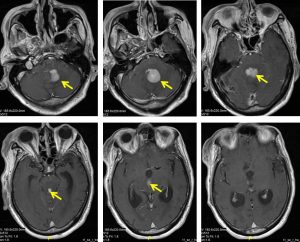
- It shows isointense signal on T1, heterogeneous hyperintense on T2 and not suppressed on FLAIR. Homogenous avid enhancement is seen post IV Gadolinium.
- There is extension of the mass enhacement along the ventricles superiorly to third ventricle region.
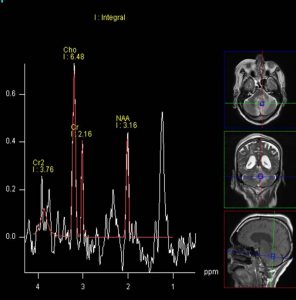
- Low NAA with reverse choline creatine ration is demonstrated on MR spectroscopy. Lactate lipid peaks are also seen.
- No blooming artefact is identified on GRE sequence to suggest presence of calcification or hemosiderin-containing chronic blood product.
- Associated marked perilesional white matter oedema is seen.
- Third and lateral ventricle is markedly dilated with presence of periventricular T2/FLAIR hyperintensities; suggestive of obstructive hydrocephalus.
- No focal intraventricular lesion is seen within the lateral ventricles. Choroid plexuses are normal in appearance.
- No midline shift or internal brain herniation. Basal cisterns and sulci are not effaced.
HPE findings:
- Macroscopy: specimen labelled as brain tumour, consists of multiple pieces of whitish tissue.
- Microscopy: sections show multiple fragments of hypercellular tumour tissue composed of medium sized to large lymphoid cells arranged in diffuse sheets. The cells display pleomorphic, round to ovoid, vesicular to hyperchromatic nuclei, prominent nucleoli and scanty neoplasm. Mitosis is brisk with numerous apoptotic cells. Areas of necrosis are prominent. Perivascular aggregates of tumour cells are observed.
- Immunochemistry: The cells are positive to CD20 and vimentin. the lymphoid cells are positive for CD20, BCL6 and MUM1. The cells are negative for CD3 and CD10. The proliferative index (Ki-67) is 70-80%. Other stains: GFAP, EMA and S100 are negative.
- Interpretation: Diffuse large B-cell lymphoma
Diagnosis: Primary CNS lymphoma
Discussion:
- Primary CNS lymphoma (PCNSL) is extranodal malignant lymphoma in absence of systemic lymphoma
- In immunocompetent patient, it is usually seen in 6th -7th decades, mean age of 60 years
- Male predominance is seen
- Most common presentation is altered mental status and focal neurological deficit
- Imaging shows enhancing lesions within the basal ganglia or periventricular white matter
- 60-80% are supratentorial, 10% involved the deep gray nuclei
- Lesions cluster around the ventricles and gray white matter junctions
- It often involve and cross corpus callosum
- Frequently abut and extend along the ependymal surfaces
- Posterior fossa, sella, pineal region are uncommon
- Clasically hyperdense on plain CT with moderate, uniform enhancement
- MRI shows strong homogenous enhancement
- MRS shows reduced NAA and presence of lipid lactate peaks
Recent Comments