
Case contribution: Dr Radhiana Hassan
Clinical:
- A 45 years old man
- No known underlying illness
- Presented with reduced sharpness of vision bilaterally for 2 months
- No other symptoms.
- Clinical examination shows normal vital signs.
- Visual acuity is normal. Homonymous hemianopia detected.
- No other neurological deficit.
MRI findings:
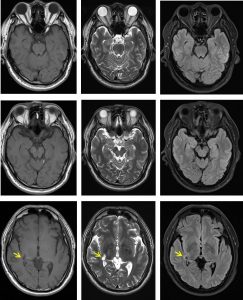
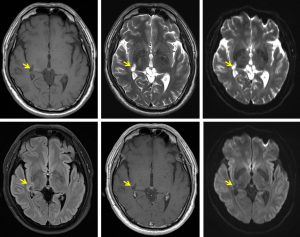
- A small well-circumscribed lesion is identified at the right corona radiata adjacent to the occipital horn of the right lateral ventricle, at the region of right lateral geniculate body.
- It appears hypointense on T1, hyperintense on T2 and suppressed on FLAIR with rim hyperintesity surrounding it. No enhancement post IV Gadolinium is detected.
- No restricted diffusion on DWI and ADC map images.
- This is in keeping with small lacunar infarction.
- Multiple lesions with T2/ FLAIR high signal intensity are seen within deep white matter at bifrontal lobes including bilateral periventricular regions most likely due to small vessel ischemia (images not shown).
Diagnosis: Infarction of right lateral geniculate body
Discussion:
- The lateral geniculate body is on the anterior third of the visual pathway.
- A lesion on this nucleus produce moderately to completely congruent visual field defect.
- Visual symptoms include a wedge-shaped homonymous hemianopia, congruent superior homonymous quadratic defect and alos a quadraple sector defect.
- The lateral geniculate body has a dual blood supply from the anterior choroidal artery (branch from ICA) and from the lateral choroidal artery (branch from PCA)
Recent Comments