")
Case contribution: Dr Radhiana Hassan
Clinical:
- A 57 years old with underlying hypertension and diabetes mellitus
- He presented with presyncopal attack, giddiness and vomiting
- Later on had loss of consciousness
- No fitting episode and no fever
- Urgent CT scan brain was normal
- Initially treated as acute myocardial infarction
- However his condition deteriorated and a repeat CT scan brain was performed.
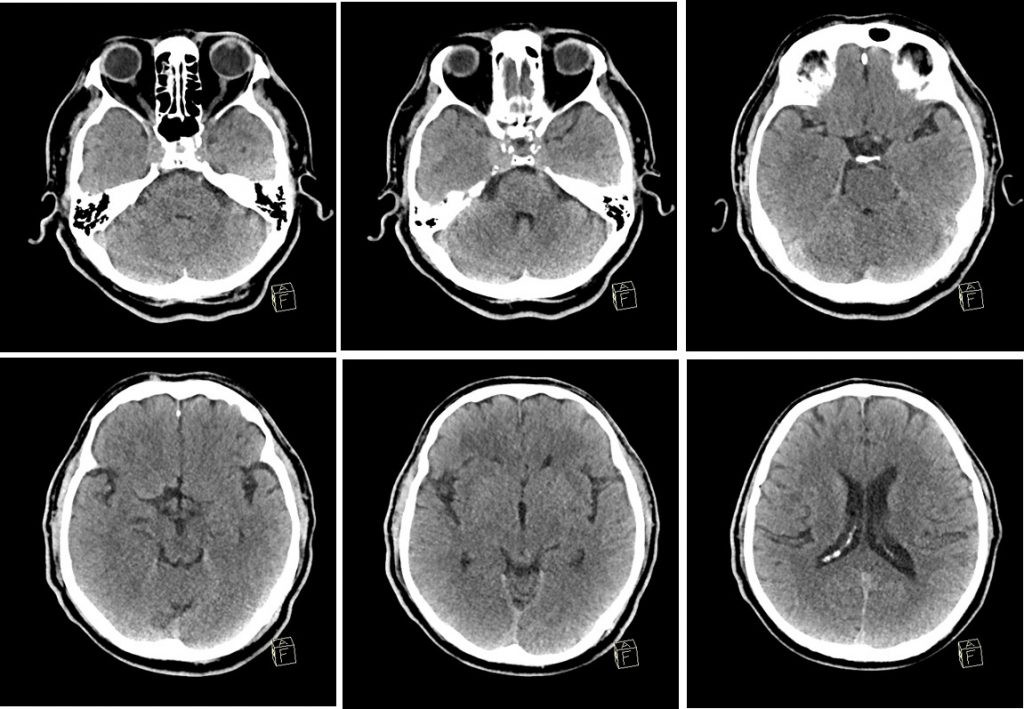
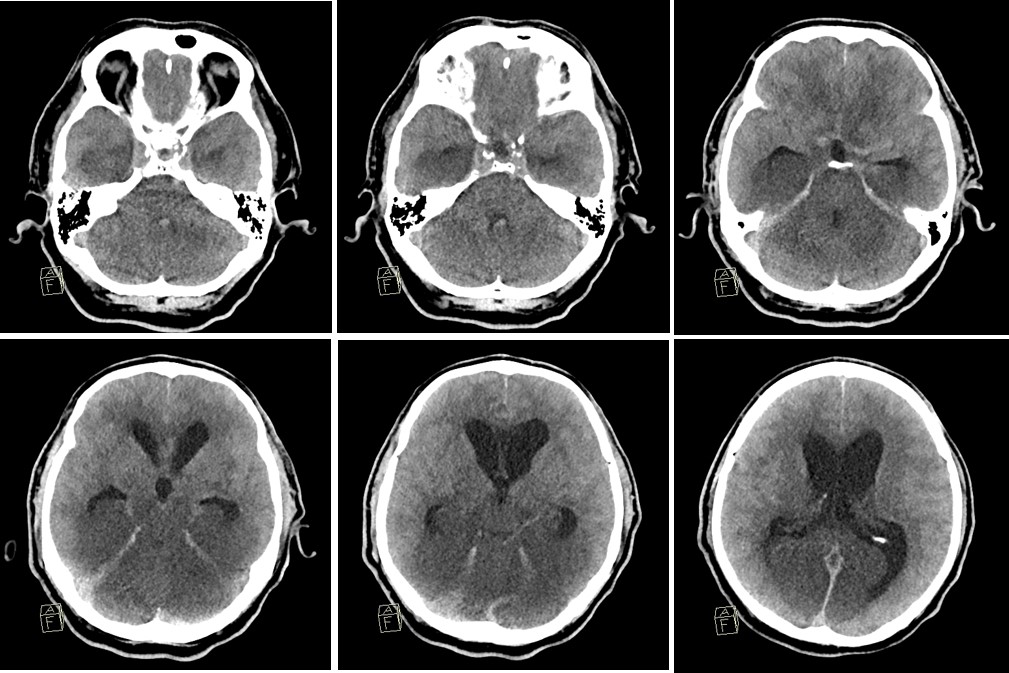
CT scan findings:
- Acute communicating hydrocephalus with effacement of cerebral sulci
- Extensive hypodensities seen in the brain stem, both thalami, temporal and occipital lobe
- Involvement is symmetrical on both sides
- These findings are not seen on previous scan
- No intracranial hemorrhage
Diagnosis: Posterior circulation infarction (POCI)
Discussion:
- Posterior circulation infarctions represent about 20% of all ischaemic stroke
- A posterior circulation infarction is classically defined by infarction occuring within the vascular territory by the vertebrobasilar arterial system
- Atheroscleotic disease can result in thromboembolism leading to ischaemia. Large vessel atherosclerotic changes occur in about 35% of POCI and small vessel disease in 13%. Other causes include cardioembolism, arterial dissection, vertebrobasilar dolichoectasia, subclavian steal syndrome, giant cell arteritis and Fabry disease.
- Imaging shows areas correspond to vertebrobasilar vascular territory that includes
- Brain stem
- Cerebellum
- Midbrain
- Thalami
- Temporal and occipital lobe
Recent Comments