
Case contribution: Dr Radhiana Hassan
Clinical:
- A 52 years old lady, history of total thyroidectomy and appendicectomy many years ago.
- Presented with right hypochondriac pain for one week
- Gradual worsening the last 3 days, dull aching, radiated to the back
- Associated with feverish sensation.
- Per abdomen shows tenderness and mild guarded at right hypochondriac region.
- Blood investigation showed HB 10, WCC 12, PLT 392, AST 92, ALT 69, ALP 150 and TB 19.
- Imaging requested to rule out liver abscess.

Abdominal radiograph findings:
- No obvious soft tissue mass lesion
- No abnormal calcification
- Bowel loops are grossly normal
- No abnormal bone lesion seen.
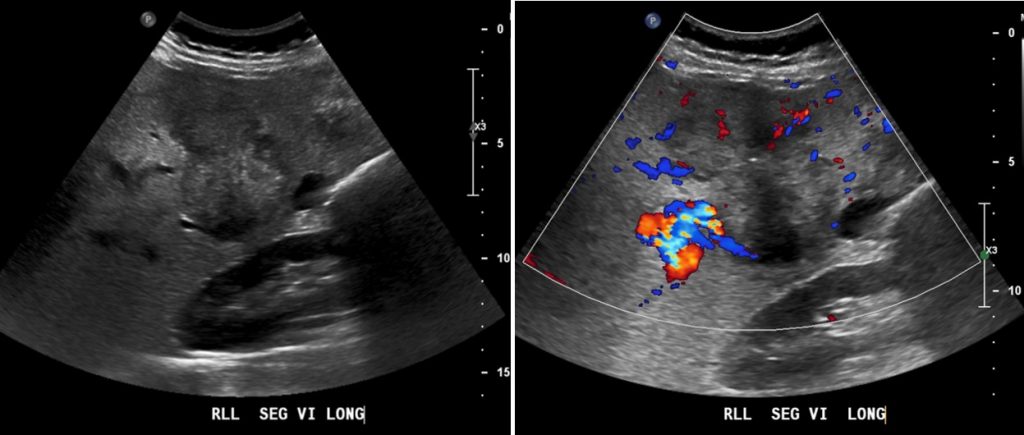
Ultrasound findings:
- The liver is enlarged measures 19.1 cm cranio-caudally at midclavicular line. The liver margin is smooth with homogenous echogenicity and echotexture.
- There is a huge, irregular, heterogenous hypoechoic liver mass seen at segment VI measuring around 7.5 x 6.3 x 8.0 cm (AP x W x CC). The intra hepatic ducts are not dilated.
- Intralesional vascularity is detected on Doppler assessment.
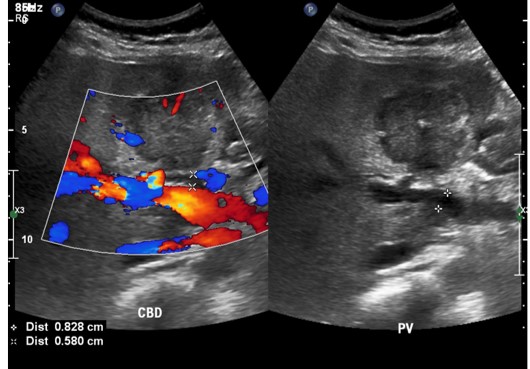
- The portal vein is patent and normal in calibre, measuring around 0.8 cm.
- The common duct is prominent measures 0.6 cm in AP diameter. The distal common bile duct is obscured by bowel gas. No obvious calculus or mass seen within the visualized CBD.
- There is a rounded cystic lesion at gall bladder fossa likely represent the gall bladder. It appears contracted with calcified thickened wall and is in closed proximity with the aforementioned liver mass.
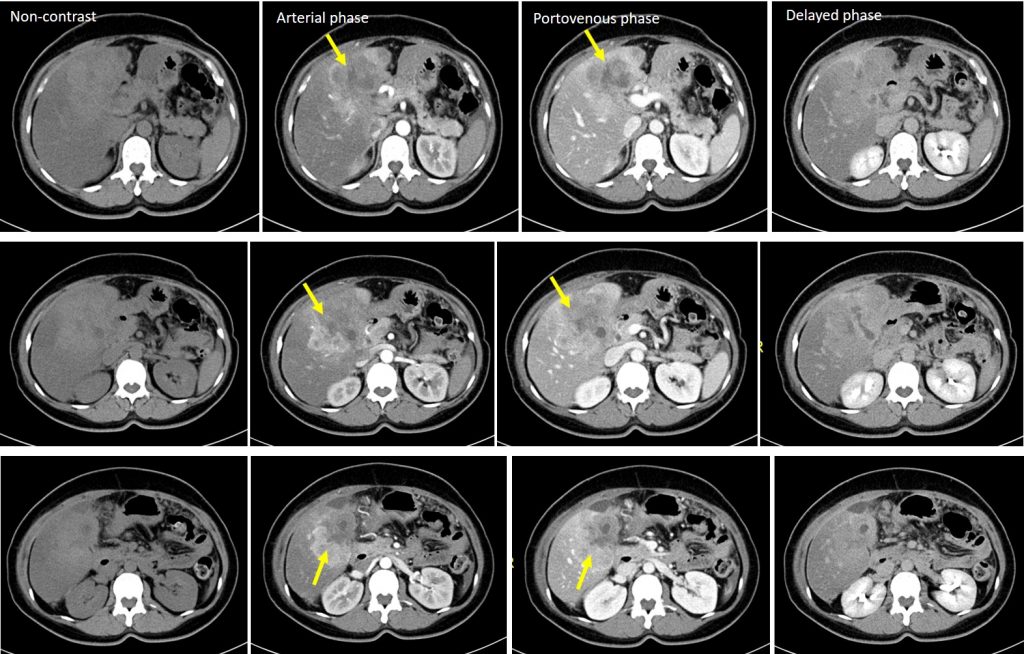
CT scan findings:
- The liver is enlarged with craniocaudal length measuring about 17.9 cm. It shows diffusely reduced attenuation (HU 2), in keeping with fatty liver. The liver margin is still smooth.
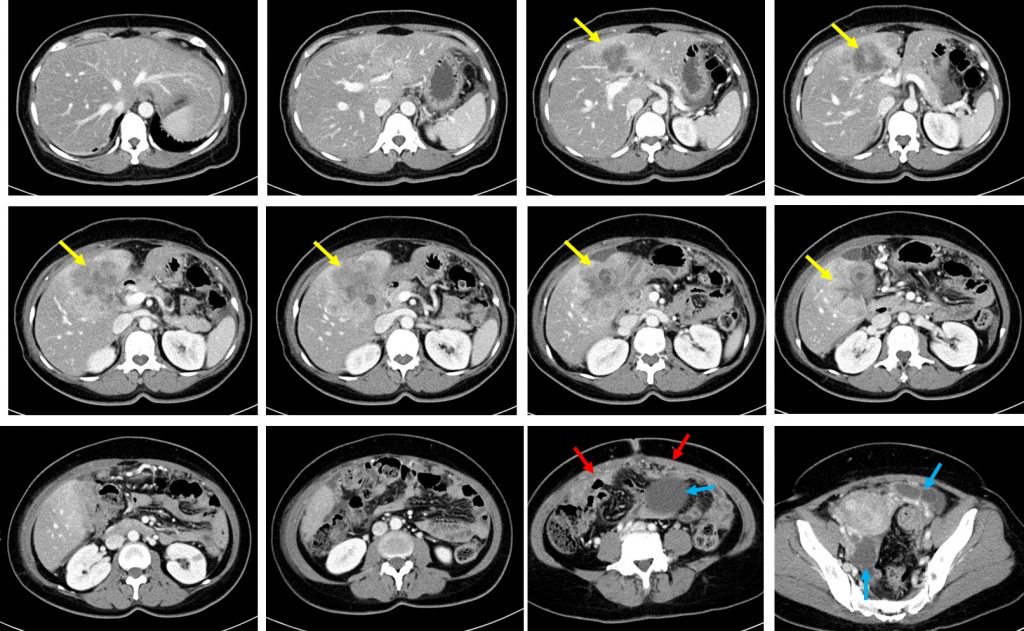
- There is a large, heterogenous mass with ill-defined margin (yellow arrows) seen involving the segment IVa, IVb and V of the liver. The mass measures about 7.3 x 8.0 x 8.0 cm (AP x W x CC).
- There is poor fat plane demarcation seen with the gallbladder. Normal configuration of the gallbladder is not visualised.
- The mass shows persistent heterogeneous contrast enhancement in arterial, portal venous and delayed phases. No significant contrast washout or centripetal filling-in observed.
- Non-enhancing hypodense areas are seen within the mass likely represent central necrosis.
- No calcification, fat component or intralesional haemorrhage.
- Portal veins and hepatic veins are patent and are not dilated.
- Some of the intrahepatic ducts in segment V are prominent measuring up to 0.3cm. The rest of the intrahepatic and extrahepatic ducts are unremarkable.
- A few enhancing peritoneal nodules are also seen at the posterior aspect of the mass (red arrows).
- There are mixed solid cystic mass seen at both adnexa which shows heterogeneous enhancement and multiple thin enhancing septations within. No ascites.
HPE findings:
- Ultrasound-guided biopsy performed.
- Macroscopy: specimen labelled as liver biopsy consist of multiple strips of tan whitish tissue measuring 7-20 mm in length.
- Microscopy: sections show three strips of fibrocollagenous tissue harbouring malignant tumour arranges as irregular glands and in areas forming cribriform pattern. The tumour cells are moderately pleomorphic, having vesicular nuclei and some have prominent nucleoli. The cytoplasm is vacuolated. In areas, hepatocytes are seen in one of the strips.
- The tumour cells are CK7 and CK20 positive.
- Interpretation: adenocarcinoma.
Progress of patient:
- Patient on palliative treatment- chemotherapy, nutrition support and analgesia
Discussion:
- Cholangiocarcinomas are malignant tumors arising from the biliary tree, excluding the gallbladder or ampulla of vater.
- Cholangiocarcinoma is the third most common primary hepatobiliary malignancy after HCC and gallbladder cancer. They tend to have a poor prognosis and high morbidity.
- They usually present in the elderly, mean age of 65 years with a slight male predilection.
- Anatomically it is classified as intrahepatic (10% of cases) and extrahepatic; perihilar (70%) and distal to cystic duct insertion (20%)
- The macroscopic appearance is described as mass-forming, periductal infiltrating or intraductal proliferating.
- Mass-forming type usually appears as an irregular but well-defined mass. This type of tumor frequently invades the adjacent peripheral branches of the portal vein and thus generally extends to the hepatic parenchyma with multicentricity around the main tumor. At later stages, mass-forming cholangiocarcinoma invades the Glisson sheath and spreads via both the portal and lymphatic systems.
- The typical CT finding of a mass-forming cholangiocarcinoma is a hypoattenuated mass with irregular peripheral enhancement in the hepatic arterial phase and gradual centripetal enhancement on dynamic studies. The peripheral portion contains abundant viable tumor cells, whereas the central portion is composed of coagulative necrosis with few cancer cells and a varying degree of fibrous stroma. The fibrous stroma in the center of the tumor is known to appear as an area of delayed enhancement on dynamic studies. Other common findings include capsular retraction, satellite nodules, and macroscopic vascular invasion.
- The MRI features of mass-forming cholangiocarcinoma are similar to the CT features. The mass typically shows high signal intensity on T2-weighted imaging and low signal intensity on T1-weighted imaging. On dynamic contrast-enhanced MRI with extracellular contrast material, the mass also exhibits prominent peripheral rim enhancement with centripetal or gradual progressive enhancement.
- On gadoxetate disodium–enhanced MR images the prominent rimlike arterial enhancement and progressive dynamic enhancement pattern are similar to those observed on MR images with extracellular contrast material. Most mass-forming cholangiocarcinomas do not take up hepatobiliary agents because of the absence of organic anionic transporter peptide expression; these tumors are thus hypointense in the hepatobiliary phase. However, mass-forming cholangiocarcinomas occasionally exhibit intermediate or mixed hyperintensity during the hepatobiliary phase because of contrast agent pooling in the fibrous stroma, which corresponds to a large extracellular space relative to normal tissue.
- A target appearance during the hepatobiliary phase is more frequently associated with in tumors with abundant central stromal fibrosis. This target sign on DWI is also useful for distinguishing cholangiocarcinoma from hepatocellular carcinoma (HCC).
- Several imaging features in favour of cholangiocarcinoma to differentiate from HCC includes a lobulated shape, rim enhancement during the arterial phase, and a target appearance with a peripheral hyperintense rim on DWI
- On the other hand, MRI findings such as intralesional fat, diffuse hyperintensity on unenhanced T1-weighted imaging, nodule-in-nodule appearance, and capsular appearance during the portal venous or transitional phase are suggestive of HCC rather than cholangiocarcinoma.
- Hepatobiliary phase imaging of gadoxetate disodium–enhanced MRI provides additional value in the differentiation between cholangiocarcinoma nd HCC. On hepatobiliary phase images, 75.0–85.7% of cholangiocarcinomas showed a multilayered pattern with hypointense rim, whereas HCCs typically showed homogeneous hypointensity.
- In addition, although only 5–12% of HCCs exhibit diffuse hyperintensity in the hepatobiliary phase, this feature rarely occurs in cholangiocarcinoma, so the presence of this feature favors a diagnosis of HCC over cholangiocarcinoma.
Recent Comments