
Case contribution: Dr Radhiana Binti Hassan
Clinical:
- A 26 years old male, no known medical illness
- Presented with giddiness and headache for few days
- Associated with tremor and nausea
- No seizure, no trauma, no fever
- No neurological deficit
- Blood investigation shows infective feature
- Patient refused lumbar puncture
- CT scan and MRI brain normal
- Condition worsening, repeat MRI one week later
MRI findings:
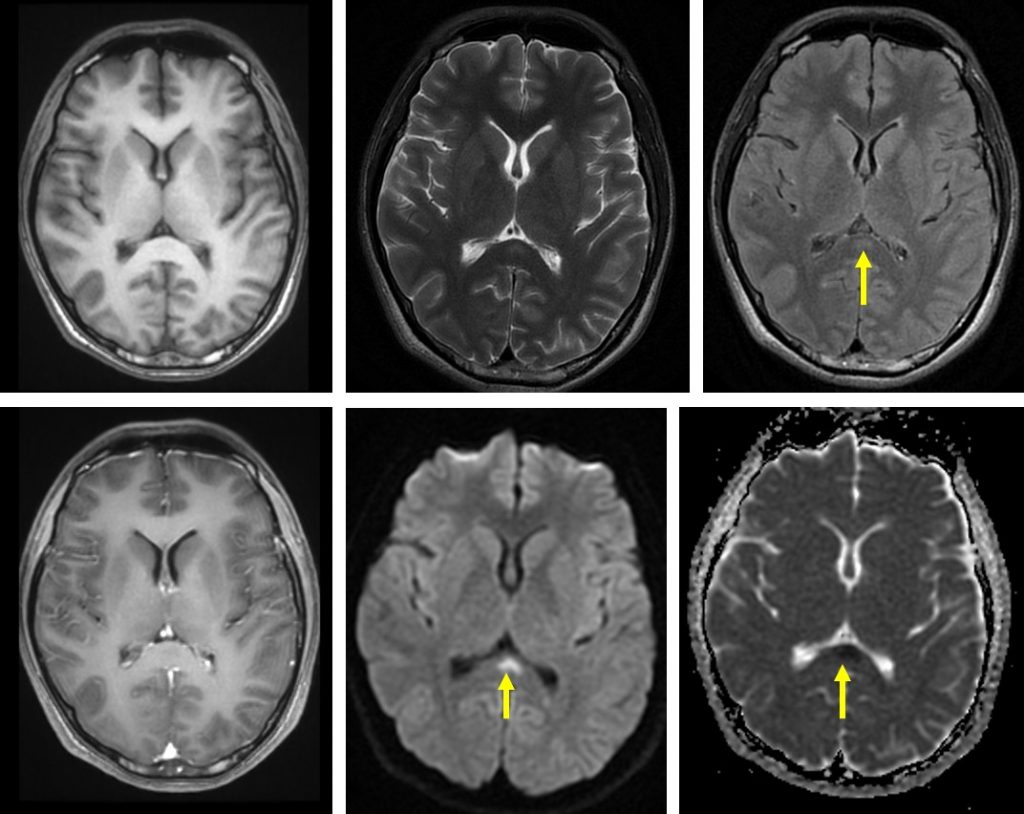
- An area of abnormal signal within the splenium of corpus callosum
- it is iso to hypointense on T1, subtle hyperintense on T2/FLAIR, restricted diffusion on DWI/ADC and no enhancement post contrast
- No expansion or swelling of the corpus callosum
- No other lesion in the brain parenchyma
- No abnormal leptomeningeal enhancement
Diagnosis: Focal cytotoxic change in splenium of corpus callosum most likely due to encephalitis
Progress:
- Patient was treated with antibiotic empirically
- Shows improvement in clinical condition
Discussion:
- The splenium of the corpus callosum connects occipital, parietal, inferior and medial temporal cortex region.
- The splenium obtains arterial supply from posterior cerebral artery (PCA).
- Focal imaging abnormalities of the corpus callosum are rare and have been described in a variety of neurological disorders.
- The splenium of corpus callosum is preferentially affected by cytotoxic changes seen due to presence of a high density of oligodendrocytes expressing large numbers of glutamate affected receptors.
- The wide variety of clinical causes include:
- Seizures: sudden cessation of antiepileptic, seizures with or without medication
- Metabolic disturbance: hyperammonia, hyponatremia, hepatic encephalopathy, hypoglycaemia, Marchiafava-Bignami disease, osmotic demyelination, Wilson disease
- Encephalitis: viral such as measles, herpes, rotavirus and SARS-CoV, bacteria and mycobacterial
- CNS malignancy
- Imaging findings to of this on MRI is hypointense or isointense on T1WI, hyperintense on T2 and FLAIR with no enhancement on post contrast images. It shows restricted diffusion in DWI/ADC sequences>
- It is typically seen as round or oval shaped restricted diffusion, centrally located in the splenium of the corpus callosum.
- To differentiate this condition with Marchiava-Bignami disease, usually the latter is more extensive, symmetrical hyperintensity and swelling of parts or whole corpus callosum extending into the adjacent white matter sparing the subcortical U-fibers (boomerang shaped area of restricted diffusion)
- Ischaemic stroke is another very rare differential diagnosis. On imaging it is seen to be more irregular in shape and eccentric in location.
Recent Comments