
Case contribution: Dr Radhiana Hassan
Clinical:
- A 58 years old man with underlying DM, hypertension and hyperlipidaemia
- Presented with high grade fever, chills and rigor for 5 days
- Associated with poor oral intake
- No URTI symptoms
- No UTI symptoms
- No rashes, No history of contact with COVID-19 patients
- WBC: 5.7, CRP=26.8, Mantoux test –ve, CXR normal
- ECHO no vegetation, US abdomen normal, Dengue serology –ve, Blood C&S Burkholderia pseudomallei
CT scan findings:
- CT scan was performed to look for occult abscesses as CXR and US were normal
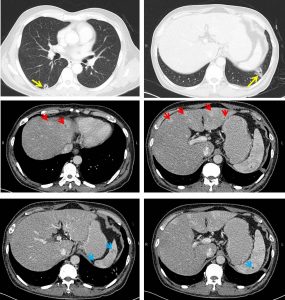
- CT scan shows a few cavitating lesions in both lungs (yellow arrows)
- Subcentimetres mediastinal nodes are seen. No pleural effusion.
- Multiple small rim enhancing lesions are also seen in the liver ( red arrows) and spleen ( blue arrows). NO similar lesion in the prostate gland.
- No ascites, no abnormal enlargement of paraortic or paracaval nodes
Diagnosis: Meliodosis
Discussion:
- Melioidosis is an infection caused by Burkholderia pseudomallei
- Melioidosis most commonly infects adults with an underlying predisposing condition, mainly diabetes mellitus.
- Melioidosis has a wide range of radiological manifestations making it a great mimicker.
- Diagnosis requires a high index of clinical suspicion in patients with septicemia or a fever of unknown origin living in or with a travel history to endemic areas.
- Almost every organ can be affected.
- Pulmonary manifestation include small nodules, typically affecting the upper lobes that may rapidly progress in cavitation or pulmonary abscess formation. Pleural effusions are uncommon.
- Head and neck manifestation includes suppurative parotitis.
- Abdominal manifestation most commonly involving the liver and spleen. Pancreas, kidneys and prostate glands are other organ that can be affected.
- CNS involvement is uncommon, ranging from cerebral abscess, cerebritis and dural venous thrombosis
Recent Comments