
Clinical:
- A 30 years old man
- Chest radiograph performed after insertion of central venous catheter
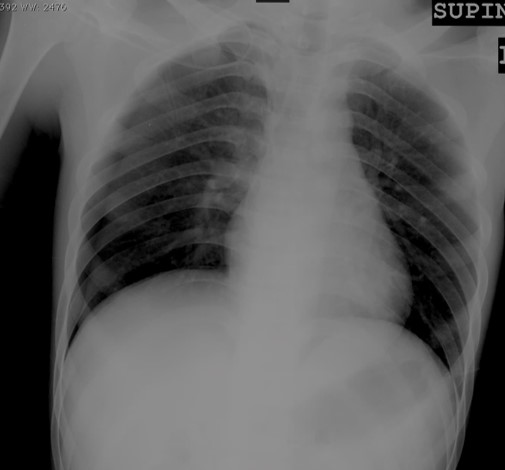
Radiographic findings:
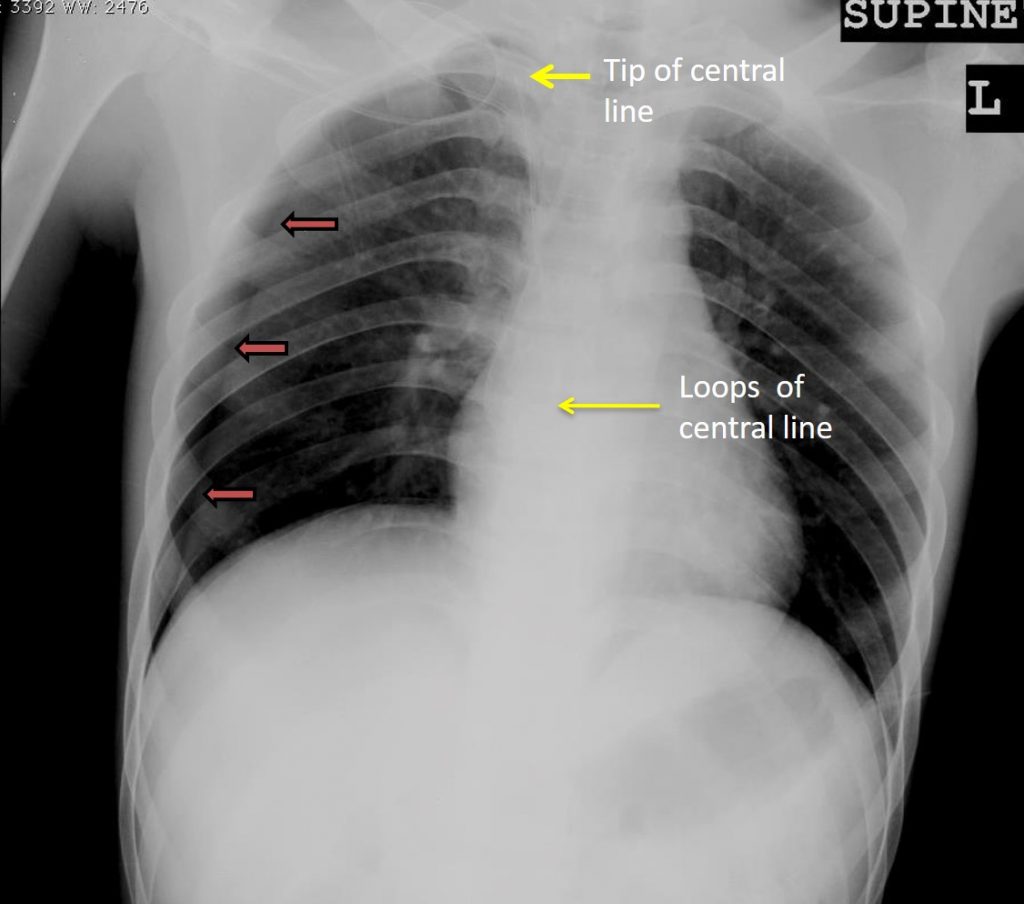
- Visualization of pleural lining on the right side (orange arrows) with no lung markings distal to this pleural lining in keeping with pneumothorax
- No mediastinal shift or flattening of hemidiaphragm to suggest tension pneumothorax
- The central line is seen forming a loop at atrial region and its tip seen over the upper mediastinal area (yellow arrows)
- No blunting of both costophrenic angle
Diagnosis: Iatrogenic right pneumothorax post central venous catheter insertion
Discussion:
- The central venous catheter is a catheter placed into a large veins such as internal jugular vein, subclavian vein or femoral vein.
- Pneumothorax is the one of the most frequent mechanical complications during central venous catheter (CVC) insertion.
- The incidence of pneumothorax varies between 1% and 6.6%.
- Higher incidences seen in the following situations: emergency situations, large catheters size, catheters used for dialysis, and with the increased number of needle passes.
- It was a common practice to exclude radiologically detectable complications after the insertion of CVCs by the jugular or subclavian approach by chest X-ray
- However, recently many authors found no value in routine X-ray after CVC placement.
- Supine chest radiographs were unreliable in making the diagnosis of pneumothorax, with a sensitivity value of 36%.
- Supine chest radiograph is not sensitive to identify hidden pneumothorax because the air initially dissipates within the non-dependent and medial parts of the chest and therefore can be invisible on supine radiographs.
- Clinician-performed bedside US has been reported to be superior to supine chest radiograph for detection of pneumothorax.
- CT thorax is sensitive and accurate, however it involves radiation exposure; and its increased cost makes it an inefficient screening tool.
Recent Comments