
Clinical:
- An 14 years old girl
- Presented with central precocious puberty since infancy
- Also had epilepsy on antiepileptics and psychosis on treatment
- Operation done at one year of age
- HPE confirmed hypothalamic hamartoma.
- MRI for reassessment

MRI findings:
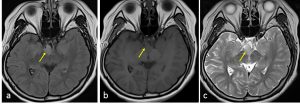
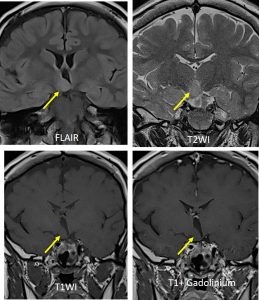
- The is an ovoid mass arising from the right side of the hypothalamus/tuber cinereum (yellow arrows)
- The lesion measures 1.7 x 1.5 x 1.6 cm, no change compared to previous scan
- This mass is isointense to grey matter in all sequences. There is no significant enhancement seen post gadolinium.
- The mass indented the 3rd ventricle anteriorly. However, it does not cause obstructive hydrocephalus.
- No compression to the optic nerve and optic chiasm
- The pituitary gland, pituitary infundibulum and the optic chiasma are normal.
Diagnosis: Hypothalamic hamartoma (HPE proven)
Discussion:
- Hypothalamic hamartoma also known as tuber cinereum hamartoma
- It is non-neoplastic congenital gray matter heterotopia in region of tuber cinereum
- Lesions can cause gelastic seizures, visual problems, early onset of puberty and behavioural problems as seen in this case
- Best imaging modality is MRI and seen as non enhancing hypothalamic mass, similar density and intensity to gray matter
- It may be sessile or pedunculated
Recent Comments