
Case contribution: Dr Khairiah Mat Nor
Clinical:
- A 52-year-old lady
- Presented with blurring of vision for 2 months associated with right facial twitching and right facial numbness.
- Clinical examination showed bitemporal heminopia (worse on the right eye) and reduced sensation over the right side of the face.
- There was no body weakness.
- CNS and cranial nerves were unremarkable.
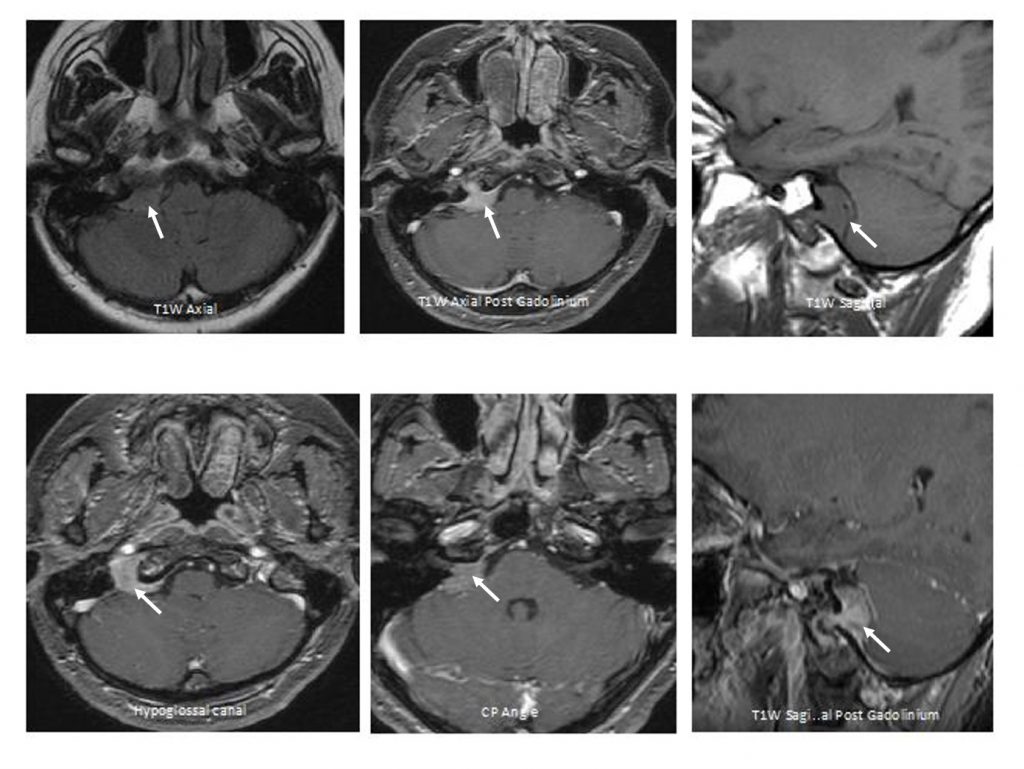
MRI findings:
- MRI of the brain and CP angle shows a well-circumscribed tubular (dumb-bell) extra-axial mass, occupying the widened right hypoglossal canal extending into the right basal cistern and encroaching the opening of right internal auditory canal (IAC).
- This mass is homogenously iso-hypointense to gray matter on T1 and T2-weighted sequences. It enhances homogenously post contrast.
- It measures approximately 1.7 (AP) x 2.3 (Wt) x (Ht) cm of the cisternal portion.
Diagnosis: Right hypoglossal schwannoma
Discussion:
- Hypoglossal nerve is the 12th cranial nerve of motor denervation for both intrinsic and extrinsic muscles of the tounge.
- The hypoglossal nerve schwannoma is very rare. It accounts for 5% of all non-acoustic intracranial schwannomas.
- Intracranial hypoglossal schwannoma usually passes through the hypoglossal canal to extends extracranially, causing widening of hypoglossal canal thus, giving a “ dumbbell-shaped” appearance.
- The clinical presentation of hypoglossal schwannoma varies, from ataxia to vertigo or facial nerve palsy and palsy of the tongue. Hypoglossal nerve palsy, is not pathognomic of the disease, absent of hypoglossal nerve palsy have been reported.
- Most schwannomas are large tumours, therefore its extension into the cerebellopontine angle is commonly seen, with or without compression onto the cerebellum, the brain stem or the 4th ventricle.
Recent Comments