
Case contribution: Dr Radhiana Hassan
Clinical:
- A 22 years old lady
- Presented with non-productive cough for one month
- Also has shortness of breath on exertion for 2 weeks
- Associated loss of weight about 7 kg in one month
- Clinically examination shows two masses at left anterior chest wall measuring 6x7cm and 10x8cm.
- Elevated Ca125: 233 U/mL.
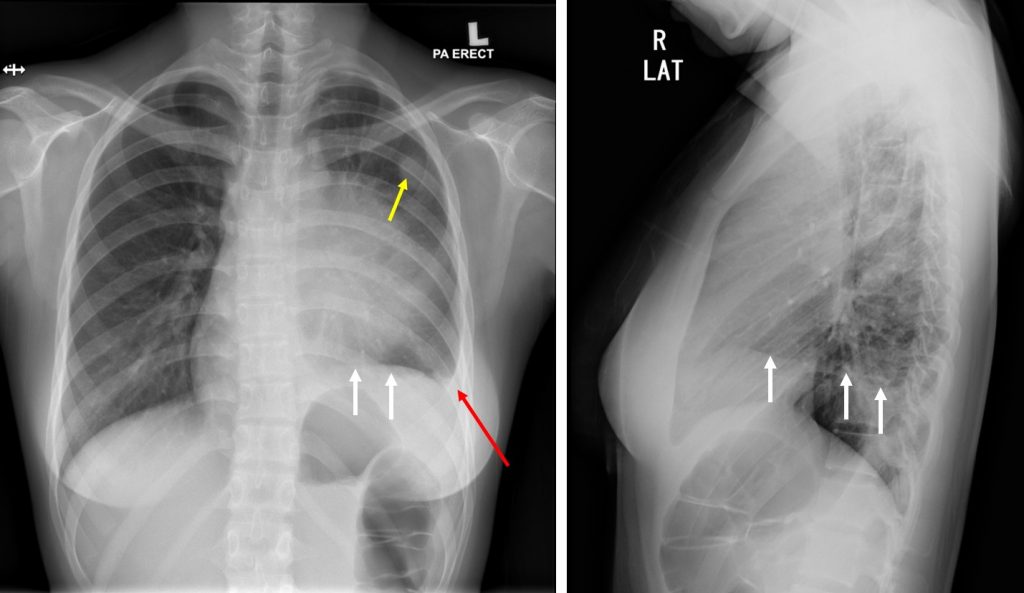
Radiographic findings:
- There is a large mediastinal mass
- The lesion is obscuring the left heart border and left hilum
- No intralesional calcification seen. No fluid levels within.
- There is elevation of the left hemidiaphragm (white arrows)
- Blunting of left costophrenic angle (red arrow)
- Another smaller well defined radio-opaque lesion is seen at left upper zone (yellow arrow).
- Right lung is clear. No right pleural effusion.
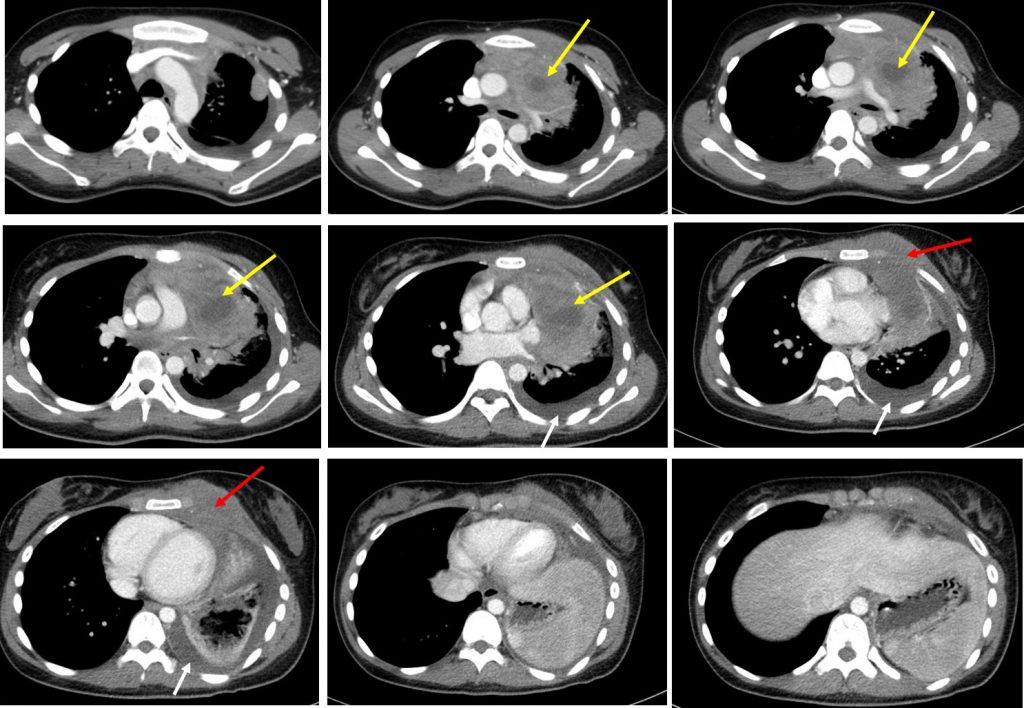
CT findings:
- There is a large mass seen at the anterior mediastinum (yellow arrows) which extends mainly to the left side. It shows a heterogenous enhancement with central hypodensity suggestive of central necrosis. It measures about 7.9 AP x 5.1 W x 9.5 cm CC.
- The mass is seen encasing the left brachiocephalic vein, main pulmonary trunk, left pulmonary artery until the hilum and both left pulmonary veins. It also abuts the arch of aorta and a large part of the descending thoracic aorta with no clear plane of demarcation.
- Anteriorly, the mass is seen in close approximity with the left anterior thoracic wall muscles with no clear plane of demarcation. There is tumor extension into the left pectoralis major (red arrows).
- No associated breast lesion seen. No erosion of the ribs. No suspicious lytic or sclerotic bone lesion.
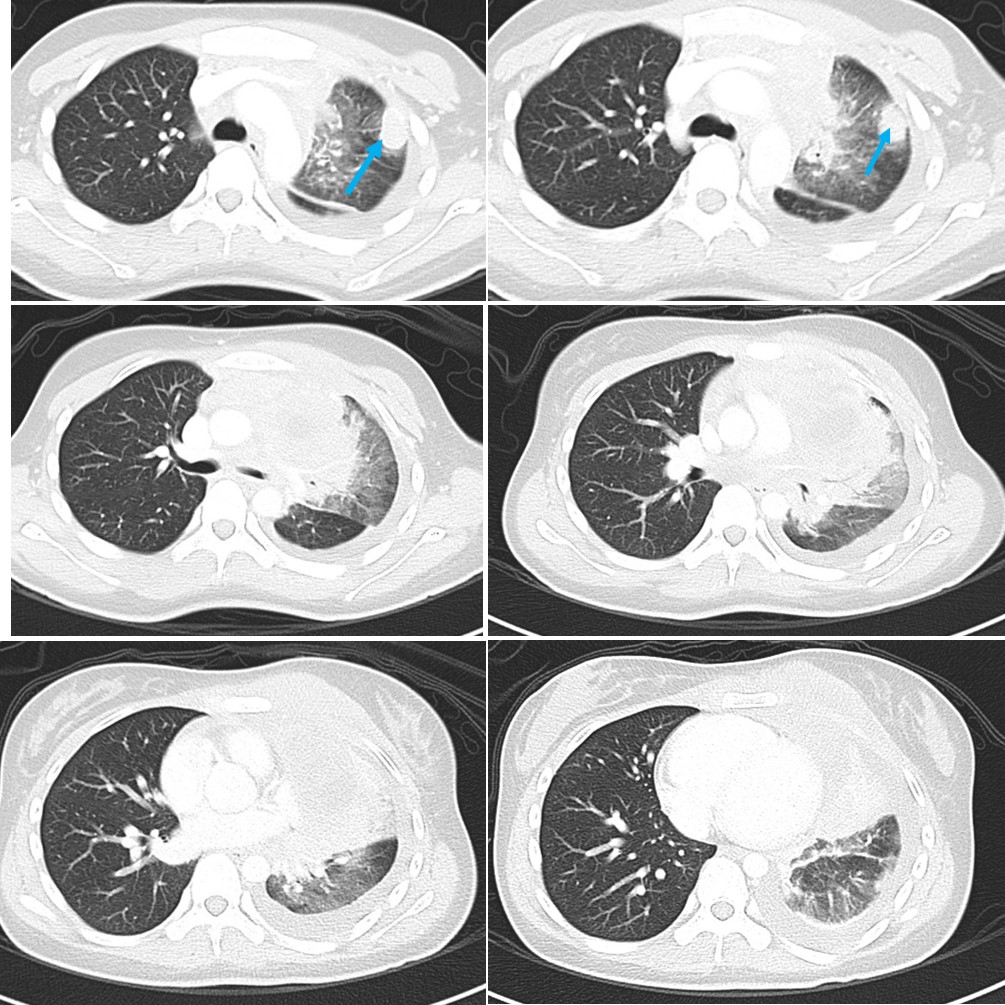
- Patchy ground glass opacity is seen at the left upper and lower lobes with some air bronchograms within, suggestive of infiltration or consolidations.
- A small lobulated lesion is seen at the apicoposterior segment of left upper lobe measures about 2.1 AP x 1.5 W x 2.1 cm CC (blue arrows).
- No pleural based nodule seen.
- Multiple enlarged mediastinal nodes.
- Left pleural effusion (white arrows) with fluid in the left oblique fissure is seen.
- Segmental left lower lobe collapse is also seen.
HPE findings:
- Macroscopy: specimen labelled as endobronchial biopsy.
- Microscopy: section shows fragments of fibrocollagenous tissue partly lined by benign respiratory type epithelium with extensive crushed artifact seen. The stroma is diffusely infiltrated by malignant lymphoid cells. The malignant cells display medium to large in size, pleomorphic nuclei, hyperchromatic to vesicular nuclei with some shows prominent nucleoli. Occasional mitosis is seen. Areas of necrosis is noted.
- Immunohistochemical studies shows the malignant cells CD20 positive and CD3 negative.
- Interpretation: Suggestive of B-cell lymphoma
Discussion:
- Mediastinal mass may be caused by a wide variety of neoplastic and non-neoplastic pathologies.
- The differentials include 5Ts;
- thymus tumour
- thyroid mass (retrosternal)
- mediastinal teratoma (germ cell tumour)
- mediastinal lymphoma
- thoracic aneurysm
Recent Comments