
Clinical:
- A 65 years old man
- Complaint of blurring of vision of left eye for the past 2 weeks
- Patient also complaints of vomiting and nausea
- Also had bilateral nose blocked with associated anosmia
- Loss of weight and loss of appetite
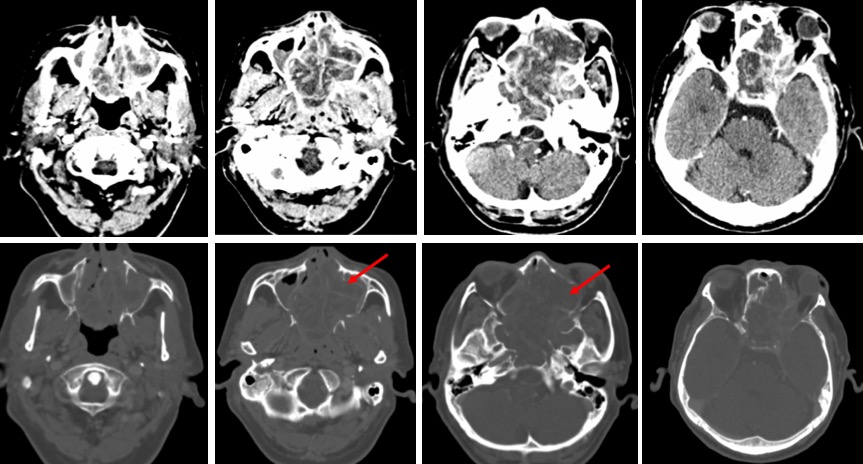
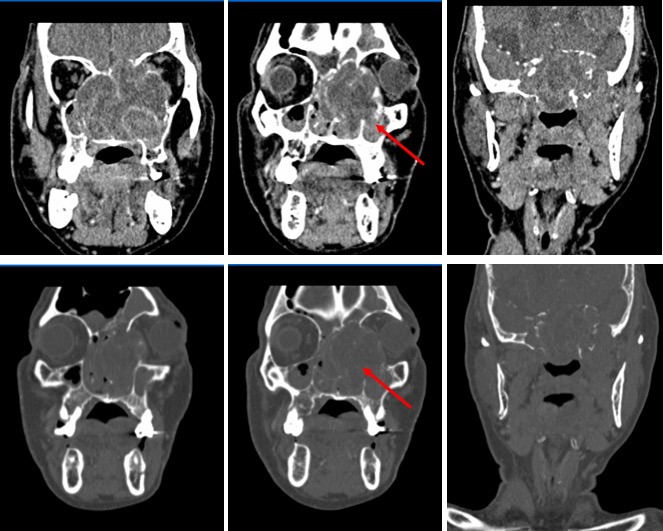
CT scan findings:
- CT scan revealed a heterogeneously enhancing infiltrative soft tissue lesion occupying the left ethmoidal sinus (red arrows).
- Medially, it crosses the midline to involve the right ethmoidal sinus.
- The lesion is extending into nasal cavity and eroding the walls of the sinus.
- It also causing scalloping of the medial wall of left orbit with resulting proptosis. The mass abuts the left medial rectus muscle.
- There is extension into the left orbital cavity, however no obvious evidence of any intra cranial or skull base extension was seen.
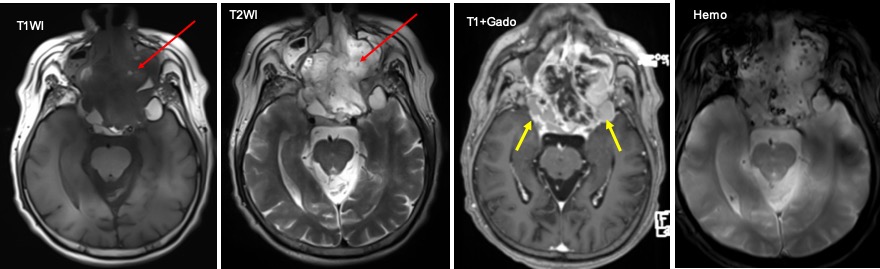
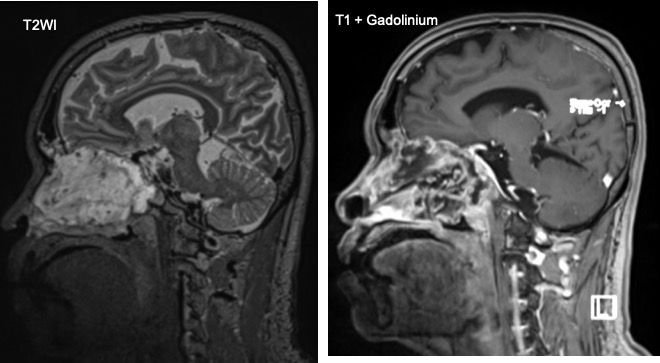
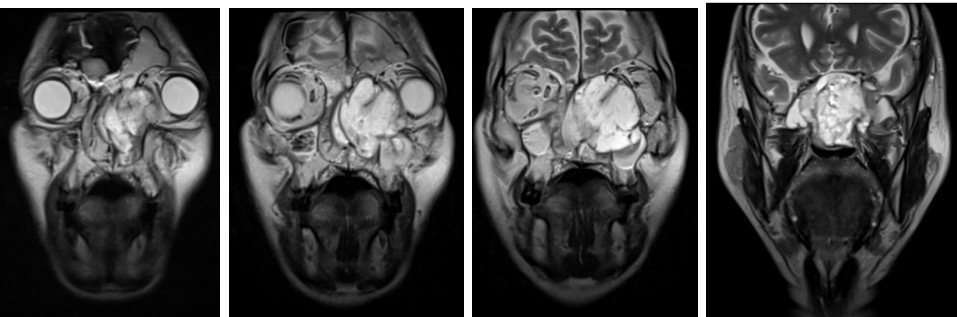
MRI findings:
- There is a large lobulated mass lesion with epicenter of the mass at the left ethmoidal sinus
- Left laterally, the mass pushes the left globe anterolaterally; left proptosis is noted.
- It extends into the extraconal space of the left orbit. The left inferior and medial recti muscles are displaced laterally by the mass. No clear fat plane between these muscles and the left lateral margin of the mass.
- The mass breaches the floor of the left orbit, extending into the left maxillary sinus causing obstruction with fluid retention noted within.
- Anteriorly the mass compresses the left nasolacrimal duct.
- Superiorly, the mass elevates the floor of the anterior cranial fossa, more markedly on the left, and the left fovea ethmoidalis is demineralised and elevated.
- No focal enhancing lesion seen in the brain parenchyma.
- The left fronto-ethmoidal recess is obstructed, with fluid retention within the left frontal sinus. The mass extends into both cavernous sinuses and elevates and encases both intracavernous internal carotid arteries. Both Meckel caves remain intact.
Diagnosis: Adenoic cystic carcinoma of ethmoidal sinus (HPE proven)
Discussion:
- Adenoid cystic carcinomas are rare malignant tumours, which represents less than 0.15% of all malignant head and neck tumours regardless of site and histology.
- It usually arise in the major and minor salivary glands, but can occur in all sites comprising secretory glands (breast, cervix, colon, prostate).
- Paranasal sinus involvement are associated with a poorer prognosis.
- The average age at presentation is the fifth to sixth decade of life.
- The maxillary sinus is the most commonly affected primary site, followed by the nasal cavity, ethmoid sinus, and sphenoid sinus
- It tends to recur locally with ‘skip lesion’ neural involvement.
- Adenoid cystic carcinomas are tumours with slow and insidious growth, often discovered at a late and locally advanced stage.
- Bone invasion (41%), perineural invasion (40%), and angioinvasion (3.8%) are observed in the surgical specimens of sinonasal ACCs.
- Lymph node and distant metastases are uncommon at presentation, but the reported overall recurrence rate is 56.2%.
- The most common sites of distant metastases are the lungs, followed by the liver and bone.
- It is usually seen as large irregular masses with bone destruction and heterogeneous density or signal intensity.
- This lesion shows isointensity on T1WI and iso- to hyperintensity on T2WI, depending on the amount of cellularity.
- It exhibit the greatest propensity for perineural spread, and the maxillary division of the trigeminal nerve is most commonly affected by sinonasal ACCs. These tumors sometimes easily extend into intracranial components including the cavernous sinus and the Gasserian ganglion, which are far away from the original site.