
Case contribution: Dr Radhiana Hassan
Clinical:
- A 33 years old lady
- No known medical illness
- Presented with jaundice 2 days associated with pale stool and tea coloured urine.
- NO fever or any constitutional symptoms.
- Previously under follow up for gastritis.
- LFT: obstructive picture.

Abdominal radiograph findings:
- There is no opacity seen overlying the right hypochondriac region
- No dilated or displacement of bowel loops.
- Normal psoas shadows bilaterally.
- No obliteration of properitoneal fat plane

Ultrasound findings:
- The common duct is dilated measuring 13 mm.
- No obvious lesion within the common duct is seen.
- No mass at pancreatic region.
- Dilatation of intrahepatic ducts are also seen (images not shown)
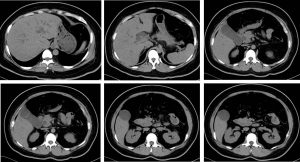
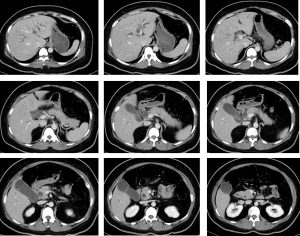

CT scan findings:
- The common bile duct (CBD) is dilated with maximal dimension measuring 1.4cm.
- The intrahepatic ducts are also minimally dilated. Smooth tapering of the CBD towards the ampullary region noted, but with no apparent hyperdense calculus detected along the CBD including at the ampullary region.
- No aerobilia observed. No intraductal lesion seen.
- No pancreatic mass detected including at the pancreatic head region.
- The pancreatic duct is not dilated.

Flouroscopy findings:
- PTBD performed with right lower segment intrahepatic duct punctured percutaneously using one step needle using biplane angiography.
- Cholangiogram shows mild dilatation of intrahepatic ducts with gross dilatation of CHD and proximal CBD.
- At least three mobile filling defects are seen within the common bile duct (yellow arrows).
- Flow of contrast seen into the duodenum on direct injection.
- An 8.3F biliary ring catheter successfully passed and secured using a suture. The distal tip is parked within the second part of the duodenum.
- No immediate complication during and immediately after the procedure. Patient vital sign is stable.Dilated intrahepatic and extrahepatic ducts secondary to choledocholithiasis.
Diagnosis: Dilated intra and extrahepatic ducts secondary to radiolucent choledocholithiasis
Discussion:
- Gallstones are common and occur in about 10% of the population
- There is female predominance (F: M = 2:1).
- The prevalence increases with age in both sexes.
- Common risk factors for cholesterol gallstones include: female sex, middle age, obesity, positive family history and recent rapid weight loss.
- Some radiopaque gallstones may be seen on plain film. However, gallstones are radiopaque only in 15-20% of cases.
- Ultrasound is considered the gold standard for detecting gallstones. It is usually seen as highly reflective echogenic focus within gallbladder lumen, normally with prominent posterior acoustic shadowing regardless of pathological type (acoustic shadowing is independent of the composition and calcium content). Gravity-dependent movement is often seen with a change of patient position.
- Calcified gallbladder stones are hyperattenuating to bile, making them the only type to be clearly visualized on CT scan images.
- Pure cholesterol stones are hypoattenuating to bile, and other gallstones are isodense to bile and these may not be clearly identified on CT.
Progress of patient:
- Removal of stones done under endoscopic procedures.
- Patient recovered well.
Recent Comments