
Case contribution: Dr Radhiana Hassan
Clinical:
- A 78 years old man
- Presented with left breast swelling for one month
- Associated with blood stained nipple discharge
- Non-tender, progressively increased in size
- No fever, no family history of malignancy
- US at other hospital shows suspicious feature (images not available)
- Biopsy shows mild atypia
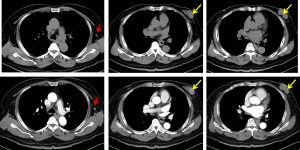

CT scan findings:
- Lobulated heterogeneous lesion is present within the left breast at lower outer quadrant (yellow arrows).
- The lesion measures 3.1 x 1.6 x 3.7 cm (AP x W x CC).
- The lesion has no internal calcification or cystic component within.
- It is surrounded with dense breast parenchyma.
- Surrounding fat streakiness and minimal overlying skin thickening observed.
- No extension into the underlying chest wall muscle.
- A few axillary lymph nodes , largest at left axilla measuring 7mm (red arrows).
- Minimal breast tissue at right retroareolar region. No mass lesion seen.
- No lung nodule or pleural effusion. No mediastinal lymphadenopathy.
- No distant metastasis (image not shown)
HPE findings:
- Macroscopy: Specimen labelled as left mastectomy. Cut section shows a well-circumscribed, firm, solid retroareolar tumour measuring 20x20x20 mm. The tumour has greyish cut surface with no hemorrhage or necrosis seen. Dense fibrous tissue are seen surrounding the tumour.
- Microscopy: sections show a tumour nodule surrounded by thick fibrous capsule, composed of delicate fibrovascular stalks, covered by a tumour cells, arranged in solid and cribriform pattern. The tumour cells display moderate pleomorphic, hyperchromatic to vesicular nuclei with prominent nucleoli. Mitosis are frequently seen. In areas, there are sheets of tumour cells infiltration outside the capsule (measuring about 7 mm microscopically) are noted. These tumour cells exhibit similar morphology as described above. There are also ductal carcinoma in-situ (DCIS) present about 5%, solid, cribriform and papillary type which are intermediate grade. No necrosis is identified. No lymphovascular invasion seen. Focal calcification are also noted. All surgical margins are free
- Immunohistochemistry, the tumour cells of invasive components are ER positive (more than 90% positive tumour cells with strong intensity) and PR positive (more than 90% positive tumour cells with strong intensity and HER 2: 2+.
- All section of total 13 lymph nodes displaying reactive lymphoid hyperplasia. Negative for malignancy.
- Interpretation: Encapsulated papillary carcinoma with invasion; TNM stage pT1bN0Mx
Diagnosis: Breast carcinoma in male
Discussion:
- Male breast cancer is a rare cancer that forms in the breast tissue of men.
- Male breast cancer is most common in older men, though it can occur at any age.
- Factors that increase the risk of male breast cancer include: older age, exposure to estrogen, family history of breast cancer, Klinefelter’s syndrome, liver disease, obesity and testicle disease or surgery.
- Men’s breast tissue has ducts and only a few if any lobules, even though they aren’t normally functional.
- Breast cancers can start from different parts of the breast. Breast cancers may begin in the ducts (ductal carcinoma), glands (lobular carcinoma) or other tissues such as lymphoma and sarcoma.
- Papillary carcinoma of the breast is a rare ductal breast cancer.
- About 50% of papillary breast carcinoma arise at retroareolar or subareolar region.
- Nipple discharge present in 22-34% of patient.
Progress of patient:
- Left mastectomy done
- Currently on T.Tamoxifen
Recent Comments