
Case contribution: Dr. Radhiana Hassan
Clinical:
- A 38 years old man
- No known medical illness
- Active smoker
- Previously under follow up for gastritis, OGDS done confirming the diagnosis
- Presented with sudden onset abdominal pain at epigastric region
- Colicky, non-radiating
- Associated with nausea and vomiting
- Clinically per abdomen distended but no peritonism

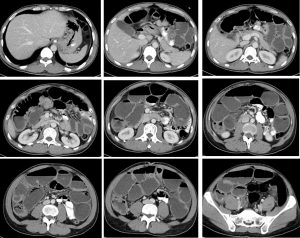
CT scan findings:
- Dilated small bowel loops are seen, mainly the small bowels
- Fluid levels are seen within the dilated bowel loops
- No obvious bowel wall thickening, no mass seen
- No free air or free fluid
- No paraortic or paracaval node enlargement
Intra-operative findings:
- Exploratory laparotomy done
- 100 cc clear peritoneal fluid, no pus, no fecal material
- Mobile constricting tumour at mid transverse colon causing dilatation of proximal colon and small bowel, distal colon appeared collapsed
- No liver nodule no peritoneal nodule
- Extended right hemicolectomy with end ileocolic anastomosis
Progress of patient:
- Complicated with anastomotic leak
- Also had enterocutaneous fistula
- HPE: adenocarcinoma, moderately differentiated TNM staging T3N1Mo
Diagnosis: Bowel obstruction due to colon carcinoma
Discussion:
- Bowel obstruction is any mechanical or functional obstruction of the intestine that prevents physiological transit and digestion.
- Colonic carcinoma is the most common cause of intestinal obstruction.
- Bowel obstruction may appear at any time during the evolution of the disease, but is more frequent in cases of advanced cancer.
- Intraluminal tumors may occlude the bowel lumen or provoke intussusception.
- Intramural infiltration through the mucosa may obstruct the lumen or impair peristaltic movements.
- Mesenteric and omental tumor involvement may angulate the bowel and provoke extramural bowel occlusion.
- Infiltration of the enteric or celiac plexus may cause severe impairment in peristalsis and consequent obstruction due to dysmotiliy.
- The radiological signs are distension of the intestinal loops, fluid retention, and gases with the presence of air-fluid levels in the zone proximal to the occlusion as well as a reduction in gas and stools in the segments distal to the obstruction. In upper occlusions, distension of the loops and air-fluid levels may be absent.
- Contrast studies such as barium enema may may be necessary to evaluate the surgical approach in certain cases.
- Computerized tomography (CT) provides a high possibility for the diagnosis of the extension of the neoplasm and on many occasions, the level of obstruction.
Recent Comments