
Case contribution: Dr. Radhiana Hassan
Clinical:
- A 46 years old man
- No known medical illness
- Ex-smoker, last smoked 12 years ago
- Right hemiparesis about one year
- Normal bowel habit, no headache, no backache, no fitting
- Vital signs are stable
- Neurological examination shows motor power right upper limb 4/5 and lower limb 3/5
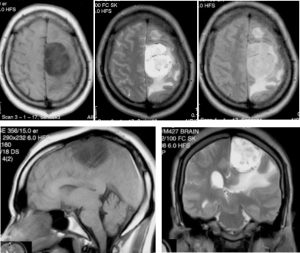
MRI findings:
- A large extra-axial tumour at parasagittal region
- It is hypointense on T1WI, hyperintense on T2WI
- Moderate perilesional oedema seen
- No contrast given during this MRI examination.
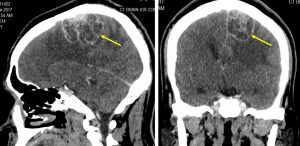
CT scan findings:
- CT scan IGS protocol for pre-operative evaluation was done
- Direct contrast scan performed.
- The mass seen on MRI shows multilobulated rim enhancement
- No dural tail sign seen
- No adjacent bone erosion or remodelling
Intra-operative findings:
- Left craniotomy and tumour excision
- Tumour was soft and well encapsulated. It was attached to the superior sagittal sinus. The tumour was moderately vascular
- the overlying dura appeared healthy.
HPE findings:
- Macroscopy: specimen labelled as brain tumour and dura consist of 2 pieces of greyish tissue.
- Microscopy: sections show tumour tissue with variably sized intercellular vacuoles or microcystic formation. There is a minor component of whorls of meningothelial cells exhibiting round to oval nuclei, inconspicuous nucleoli and indistinct border. In areas, hyalinized stromal blood vessels are seen. Mitosis is not present. Normal brain tissue is not seen. Dura sections shows hemorrhagic fibrous tissue with no invasion of tumour cells.
- Immunohistochemical staining: EMA and Vimentin positive. GFAP negative.
- Interpretation: Brain tissue: microcystic meningioma WHO Grade 1. Dura: no tumour.
Diagnosis: Microcystic meningioma.
Discussion:
- Microcystic meningioma is a rare histological subtype of meningioma, which constitutes about 1.6% of intracranial meningiomas.
- It does not show characteristic imaging features as typical type of meningioma
- The tumour is usually hypointense on T1WI and hyperintense on T2WI. Two patterns of enhancement seen on post contrast images. One is homogenous strong enhancement and another shows peripheral rim enhancement. The peripheral rim enhancement is atypical imaging feature of meningioma and may cause diagnostic confusion.
- It is associated with moderate to severe peritumoral oedema. This feature raises a clinical suspicion for more aggressive tumors, including atypical/anaplastic meningiomas, hemangiopericytoma, solitary fibrous tumor, malignant gliomas and metastatic carcinoma.
Progress of patient:
- Still having residual weakness on the right side
- However able to perform daily activities
Recent Comments