
Case contribution: Dr Radhiana Hassan
Clinical:
- A 75 years old man
- Underlying HPT, dyslipidaemia
- History of open left hernioplasty 5 years ago
- Presented with abdominal swelling for one week
- Associated with abdominal pain, colicky in nature, no constitutional symptoms, no altered bowel habit, no fever
- Clinical examination shows a left hypochondriac mass, tender, no splenomegaly
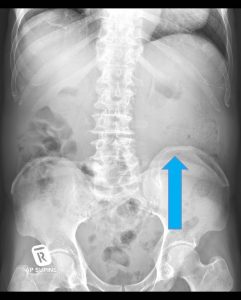
Radiograph findings:
- Soft tissue density at left lumbar region
- Paucity of bowel gas at this region
- No fluid levels or calcification within
- No dilated bowel loops
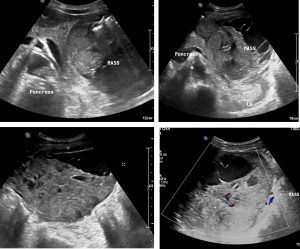
Ultrasound findings:
- There is a large heterogenous solid cystic mass occupying the left hypochondriac area.
- The cystic components have internal septations within them.
- No internal calcification seen.
- There is scanty vascularity detected on colour Doppler examination.
- The mass is seen adjacent to the tail of the pancreas and pushing the left kidney posteriorly. Otherwise the pancreas is normal.
- The mass is also seen touching the posterior margin of the left liver lobe.
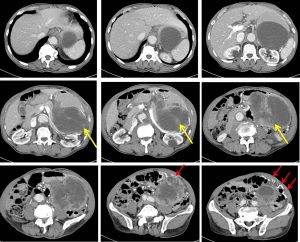
CT scan findings:
- A large heterogeneous multi-lobulated peripherally enhancing mass (mean HU 21) is seen in the left hypochondrium and lumbar region.
- This mass collectively measures about 9.8 cm x 14.7 cm x 19.2 cm (AP x W x CC).
- Large areas of central hypodensity are noted, most likely central necrosis.
- The superior part of the mass appears more cystic with HU of 18 – 30.
- Multiple vessels are also seen in between these structures, particularly at the anteroinferior aspect (red arrows).
- No fat component or calcification is seen within this mass. No fluid-fluid level is seen.
- The mass show claw-sign to the adjacent stomach, in which possible it arise from the wall of the stomach. The stomach is compressed posteriorly by the mass.
- The mass is also seen displacing the pancreas, splenic vein and left kidney posteriorly.
- The mass also displaces the bowel loops medially and inferiorly. Clear fat plane with adjacent bowel loops is seen.
- No bowel dilatation or bowel wall thickening is identified
Progress of patient:
- Tumour marker Ca19.9, AFP 3.8, CEA 1.2
- OGDS: antral gastritis
- Colonoscopy: normal
Intraoperative findings:
- Huge solid cystic mass occupying the lesser sac, pushing the stomach anteriorly and the transverse colon inferiorly
- Mass cystic in nature and highly vascularized
- Tumour densely infiltrate the posterior part of stomach at the greater curvature and tail of pancreas
- Multiple mesenteric and omentum nodules seen
- Semi-emergency laparotomy, sleeve gastrectomy and distal pancreatotomy done
HPE findings:
- Cystic tumour: gastrointestinal stromal tumour (GIST) of the stomach. TNM stage pT4pN0pM1.
- Tumour perforation is present.
- No lymphovascular or perineural invasion noted. No evidence of nodal involvement.
- Tumour deposit on the splenic capsule
- Metastatic GIST to omentum and mesenteric nodule
- Falciform ligament: no evidence of malignancy/metastasis
Discussion:
- Gastrointestinal stromal tumors (GISTs) are soft tissue sarcomas that can be located in any part of the digestive system.
- Their most common sites are the stomach and small intestine.
- The peak age for GIST of the stomach is around 60 years and a slight male preponderance is reported.
- Symptoms at presentation usually include bleeding, abdominal pain or abdominal mass.
- Endoscopically, they typically appear as a submucosal mass with or without ulceration
- on CT scans an extragastric mass is usually seen. They are rounded with frequent hemorrhage. Larger tumors may also demonstrate necrosis and cystic change. Size is variable, ranging from 1 to 30 cm.
- Typically the mass is of soft tissue density with central areas of lower density when necrosis is present (usually in larger tumors) that occasionally appear as fluid-fluid levels.
- Enhancement is typically peripheral (due to central necrosis).
- Calcification is uncommon (3%).
- Metastases (distant, peritoneal, omental) or direct invasion into adjacent organs may be seen in more aggressive lesions. Lymph node enlargement is not a feature.
- The diagnosis of malignant GIST requires histopathologic analysis, but certain characteristics suggest malignancy, which develops in 10-30% of these lesions. These include exogastric growth, diameter >5 cm, central necrosis, and extension to other organs.
Recent Comments