
Case contribution: Dr Radhiana Hassan
Clinical:
- A 56 year old lady
- para 2 with underlying hypertension.
- Presented with right breast lump for 1 month + right nipple retraction.
- Associated with loss of appetite and loss of weight
- No nipple discharge. No fever. No skin changes.
- Menarche at 13 years old and menopause at 55 years old.
- Breastfed child for 1 year.
- Clinically mass felt at right breast below the nipple, irregular and hard. No palpable lymph node.
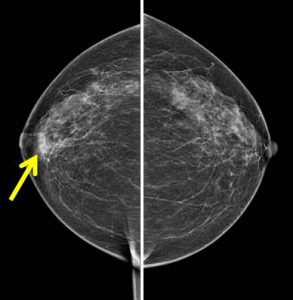

Mammogram findings:
- Moderately dense breasts with scattered fibroglandular (Birads B) breast density.
- There is focal density in the right breast at retro-areolar region(yellow arrow)
- Associated skin thickening and mild nipple retraction also seen (white arrow).
- No mass lesion and no suspicious cluster of microcalcifications.
- No stromal distortion is seen. No abnormal axillary nodes bilaterally.
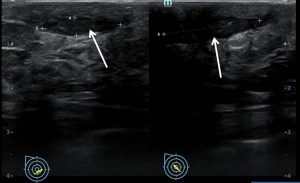
Ultrasound findings:
- At the area of complaint, there is a hypoechoic elongated lesion (Rt4H periareolar)
- It is associated with thickening of the skin adjacent to it
- The lesion appears slightly heterogenous with coarse calcification seen.
- No increase in vascularity or posterior shadowing.
- No dilated duct is identified.
- No suspicious axillary lymph node is detected bilaterally.
FNAC: Granulomatous mastitis
Progress of patient:
- Patient refused further intervention
- Claimed the lump resolved
Discussion:
- Granulomatous mastitis is a rare chronic inflammatory disease of the breast that can mimic breast carcinoma.
- The most common presentation is unilateral breast mass often associated with inflammation of the overlying skin. Nipple retraction and a sinus formation may be present. Regional lymphadenopathy is present in up to 15% of cases.
- The underlying aetiology includes infections such as mycobacterium tuberculosis, cryptococcis and histoplasmosis, auto immune process such as wagener granulomatosis and giant cell arteritis and duct ectasis.
- The imaging findings overlap with those of malignancy. The most common finding is a focal asymmetry on mammography but is is not characteristic of this disease.
- On ultrasound it is seen as an irregular hypoechoic mass with tubular extension on ultrasound.
- On MRI, a focal or diffuse asymmetrical signal intensity without significant mass effect or nodular lesion can be seen. Enhancement pattern also varies and can differ from patient to patient and from lesion to lesion.
- Core biopsy is typically diagnostic.
- Corticosteroid is the first line of treatment. Excisional biopsy is also useful.
- The prognosis is usually good but local recurrence had been reported.
Recent Comments