
Case contribution: Dr Radhiana Hassan
Clinical:
- A 41 years old male
- Underlying hypertension, fatty liver disease and DM
- Presented with sudden onset of loss of consciousness with left sided body weakness
- No trauma, no fever, no fitting episode, no vomitting
- Clinically GCS=15/15, BP=205/125mmHg, other vital signs were normal. Left hemiparesis.
- Diagnosed as hypertensive emergency
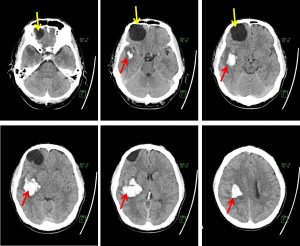
- An urgent CT brain was requested to rule out intracranial hemorrhage
CT scan findings:
- There is a large intraparenchymal hemorrhage at right frontotemporoparietal region measuring 4.4 x 4.7 x 3.7 cm (AP x W x CC) with minimal perilesional oedema.
- Effacement of adjacent right lateral sulcus.
- Midline shift to the left is noted measuring 0.5 cm.
- There are 2 well defined cystic lesions at right frontal region. They are closely attached together with cumulatively measure 3.8 x 4.3 x 4.2cm (APxWxCC).
- No calcification within the lesion
Progress of patient:
- Further examination shows ballotable right kidney
- Non tender, no other positive findings
- Patient has no genitourinary symptoms

CT scan findings:
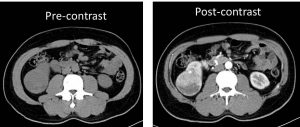
- An enhancing mass arising from the lower pole of the right kidney (white arrows) measures about 5.5 cm x 5.7 cm x 6.0 cm.
- Presence of central necrosis.
- No fat or calcification is seen within.
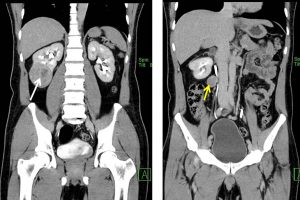
- The mass is seen touching the right Zuckerkandl fascia. However, no extension of the mass beyond this fascia is seen.
- Clear but thin plane of separation is still observed between the mass and the lateral margin of the right psoas muscle.
- A large necrotic node seen at the right renal hilar (yellow arrow) measures 2.7cm (short axis). No other enlarged abdomino-pelvic node detected.
- No renal vein or inferior vena cava thrombosis is detected.
- No hydronephrosis bilaterally.
Diagnosis: Renal cell carcinoma (presumed diagnosis) as patient refused further intervention.
Discussion:
- Renal cell carcinomas are primary malignant adenocarcinomas derived from the renal epithelium and the most common malignant renal tumour.
- It is also known as hypernephroma.
- It occurs in 50-70 years old patients.
- The most common presentation is macroscopic hematuria, flank pain and palpable flank mass
- Risk factors include cigatette smoking, dialysis-related cystic disease, obesity, hypertension and post renal transplant
- Ultrasound shows wide sonographic features and vary from solid to cystic lesion.
- On non-contrast CT, lesions are of soft tissue density with larger lesions contain areas of necrosis. About 30% demonstrate some calcification.
- On corticomedullary phase it is usually enhanced less than normal renal cortex. Larger lesions shows irregular enhancement with areas of necrosis.
- Intraluminal growth in renal vein seen in about 4-15% of cases. IVC involvement indicate worse prognosis.
Recent Comments