
Case contribution: Dr Radhiana Hassan
Clinical:
- A 47 years old lady
- Complaint of neck pain with upper limb weakness
- Worsening for the past few months
- Clinical examination shows reduced muscle power and loss of sensation at both upper limbs.
MRI findings:
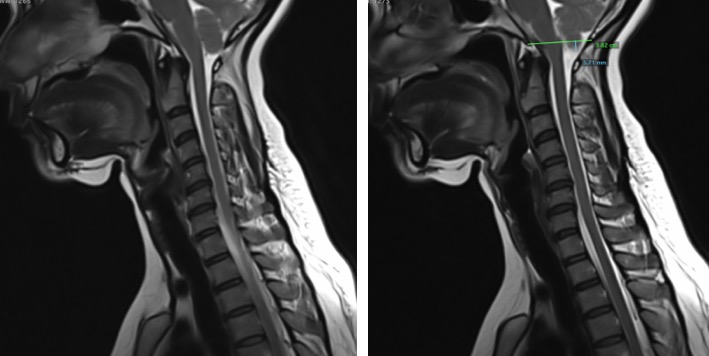
- There is inferior herniation of cerebellar tonsil about 5 mm.
- Dens is seen to be closed to the cord. No kinking of medulla.
- No syrinx formation within the cord
Diagnosis: Chiari 1 malformation
Progress of patient:
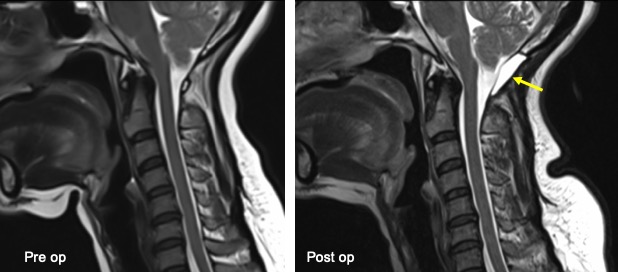
- Posterior decompression surgery was done
- MRI reassessment with new complaint of headache at rest
MRI findings:
- Suboccipital craniectomy and absent posterior atlas of C1 are consistent with previous decompression surgery.
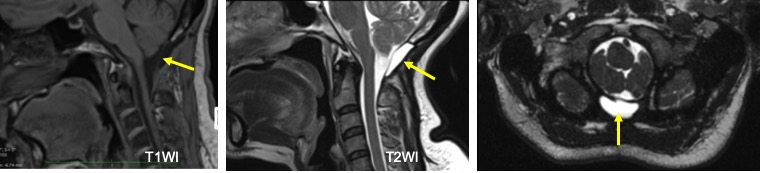
- A collection is seen posterior to the dura which is hypointense on T1 and hyperintense on T2
- The collection is well-defined, no extension to the soft tissue at neck region
- There is no discontinuity or disruption of dural layer.
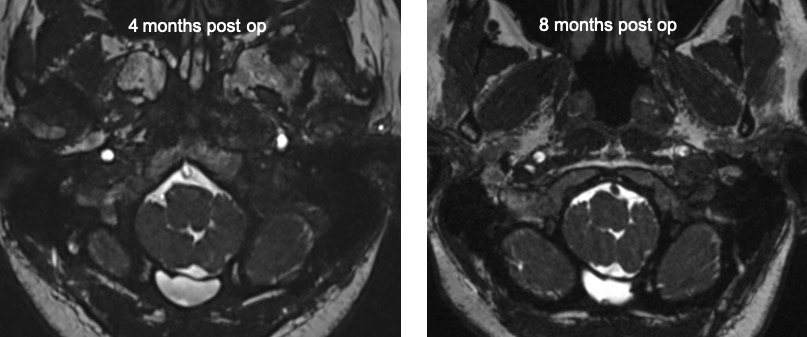
- Follow up MRI shows no increase in size of the lesion.
- The features seen are suggestive of dural sealant rather than post-operative pseudomeningocele.
Discussion:
- Chiari malformation is a developmental malformation leading to tonsillar ectopia with abnormal cerebellar tonsil morphology and tonsillar inferior descend to the foramen magnum.
- Typical imaging findings include a small posterior fossa with compression of posterior subarachnoid spaces, posterior angulation of the dens, overcrowding in the foramen magnum, peg-shaped tonsils, increased slope of the tentorium and medullary kinking.
- Surgical intervention are usually indicated for symptomatic patients. The indications include a large or progressive syrinx, headache related to coughing (tussive headache), neurological deficit ocular or otoneurologic disturbances, lower cranial nerve signs cerebellar ataxia or spasticity.
- The basic aim of surgical treatment for Chiari malformation is the restoration of normal CSF circulation at the level of foramen magnum by performing decompression of the inferior cerebellum and of the cervicomedullary region.
- The reestablishment of a pressure balance between the intracranial and intraspinal subarachnoid spaces is the main goal of all employed surgical procedures.
- Posterior fossa craniectomy , suboccipital craniectomy, removal of C1 posterior arch with or without augmentative duraplasty are among the clinical approach. Other approach include 4th ventricular stenting, endoscopic 3rd ventriculostomy, tonsillar reduction and syringohydromyelia decompression.
- Water-based dural sealants such as finrin glue, PEGH and BSAG are difficult to differentiate from CSF on standard imaging sequences.
- Differentiation is important from CSF leak due to pseudomeningoceles which are the most common complication of posterior fossa decompression.
- Recognition of water-based dural sealants therefore requires communication between the neurosurgeon and the neuroradiologist to avoid post operative misidentification.
Suggested further reading:
- Siasios et al. Surgical management of patients with chiari 1 malformation. Int J Pediatr. 2012; 640127
- Rozenfeld et al. MRI findings after surgery for Chiari malformation Type 1
- Tarapore et al. The appearance of dural sealants under MRI.
Recent Comments