
Case contribution: Dr Radhiana Hassan
Clinical:
- A 42 years old man with underlying retroviral infection
- Presented with headache and transient altered consciousness
- Clinical examination was unremarkable
- Blood investigations are normal
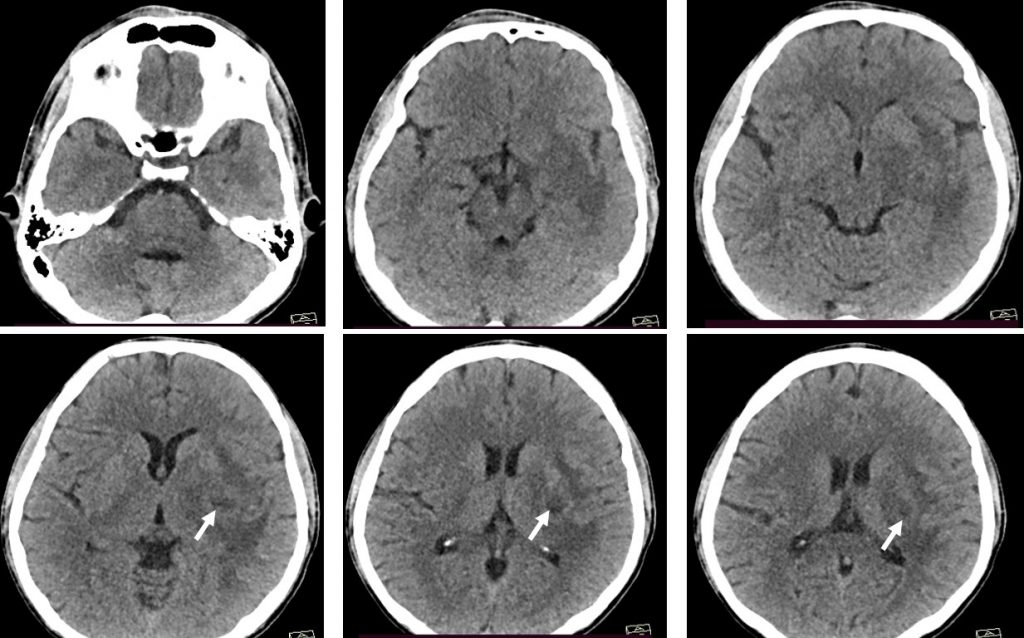
CT scan findings:
- A small lesion is seen at the left basal ganglia (white arrow)
- Itis asosciated with marked perilesional oedema
- Minimal mass effect to the ipsilateral lateral ventricle
- No midline shift. No hydrocephalus.
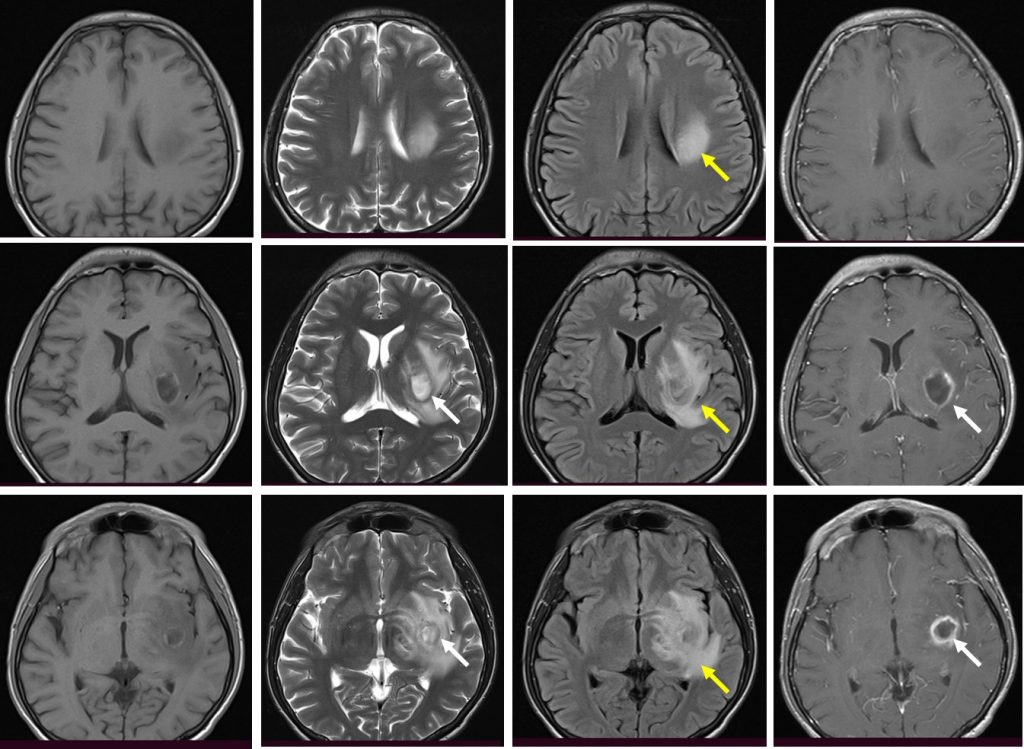
MRI findings:
- There is a lesion at left basal ganglia which is hypointense on T1, hyperintense on T2 and shows ring enhancement on post contrast
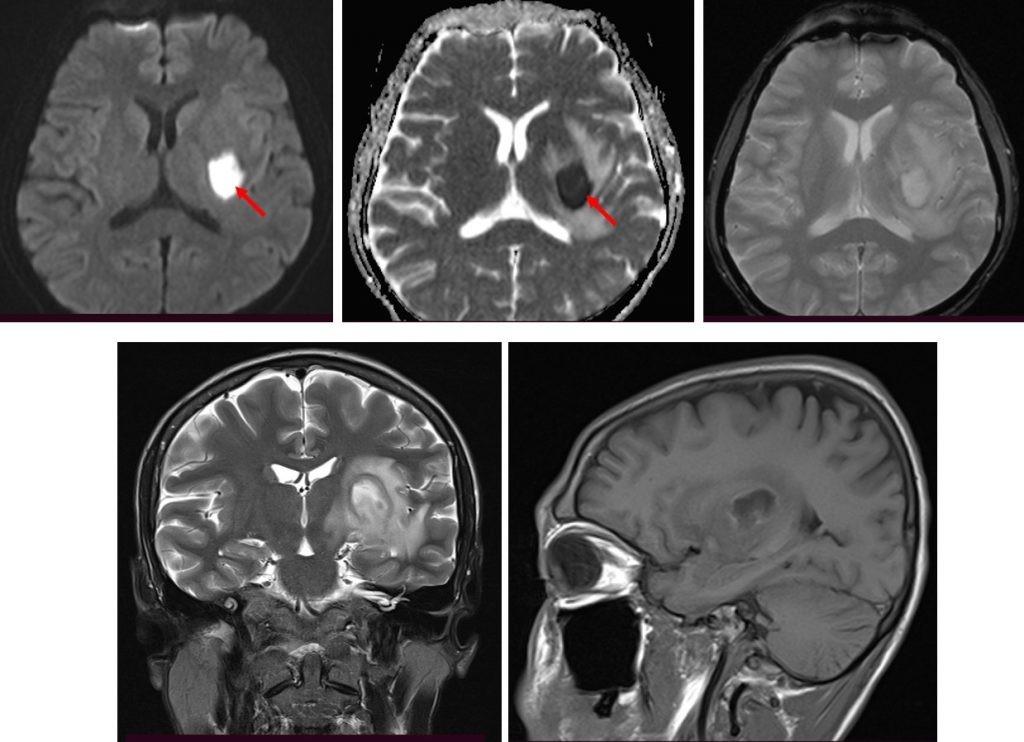
- It also shows restricted diffusion on DWI/ADC.
- Marked perilesional oedema is seen.
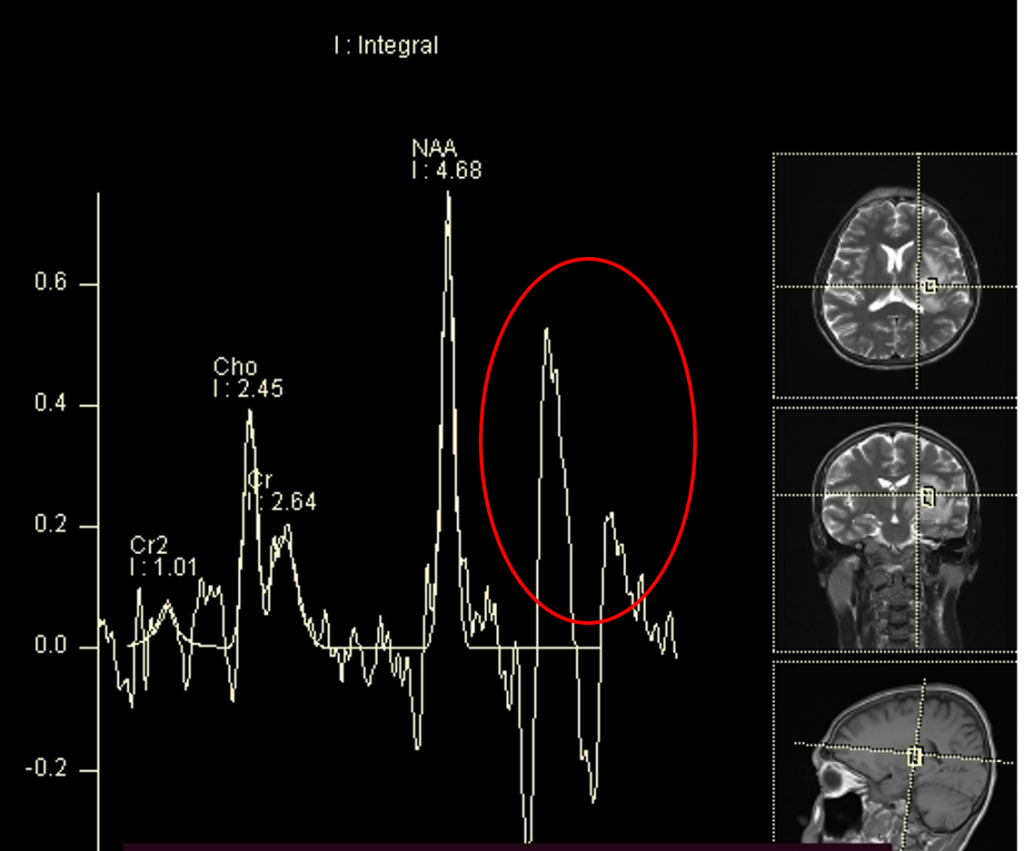
- Lactate and lipid peak are also seen on MRS
Diagnosis: Cerebral abscess.
Discussion:
- Intracranial abscesses are uncommon, serious and life-threatening infections.
- Intracranial abscesses can originate from infection of contiguous structures, secondary to hematogenous spread from a remote site, after skull trauma or surgery, and, rarely, following meningitis. In at least 15% of cases, no source can be identified.
- Imaging depends on the various stages of the disease.
- MRI is more sensitive than CT scan in the assessment of cerebral abscess.
- Differential diagnosis include metastasis, high grade glioma, subacute infarction or hemorrhage and radiation necrosis.
Recent Comments