
Case contribution: Dr Radhiana Hassan
Clinical:
- A 41 years old lady
- History of foreign body aspiration few years ago
- Diagnosed bronchitis about 10 years ago with multiple episodes of shortness of breath
- On regular nebuliser and intermittent antibiotics, no history of ICU or intubation admission
- Current presentation with chronic cough and purulent sputum for one month
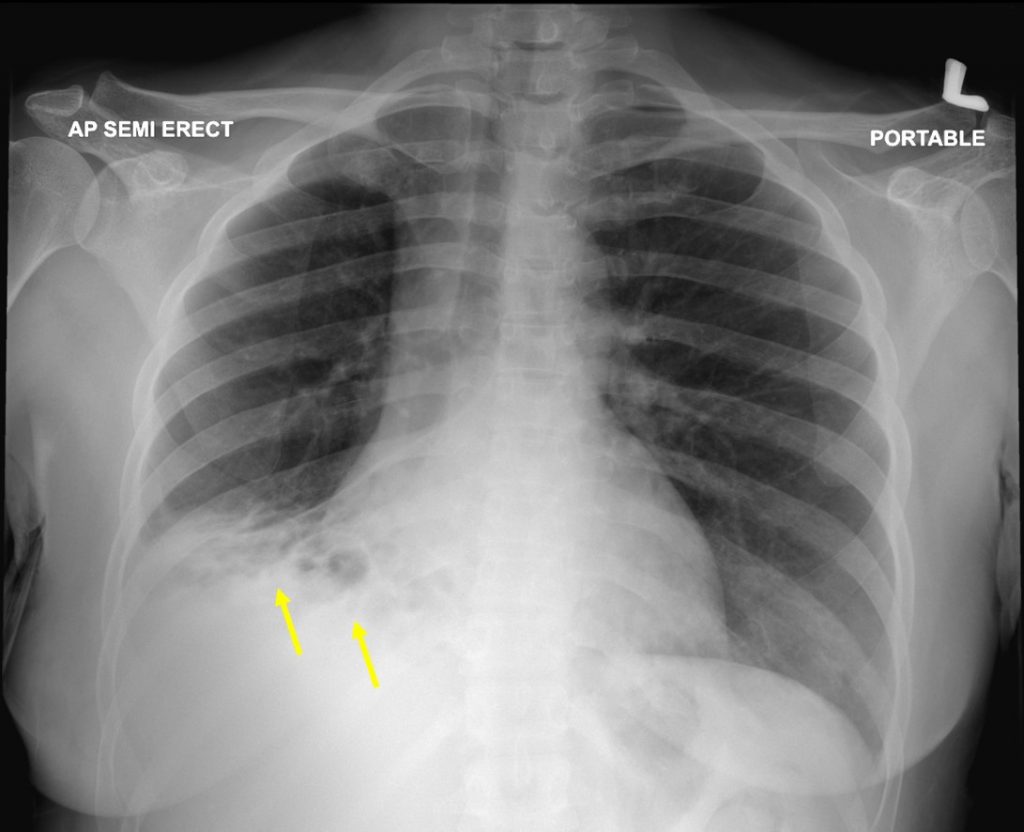
Findings of chest radiograph:
- Cystic lesion at right lower zone (yellow arrows)
- Obliteration of the right hemidiaphragm and costophrenic angle
- No obvious fluid level is seen
- No hilar mass. No other lesion in lung fields
- No abnormal bone changes
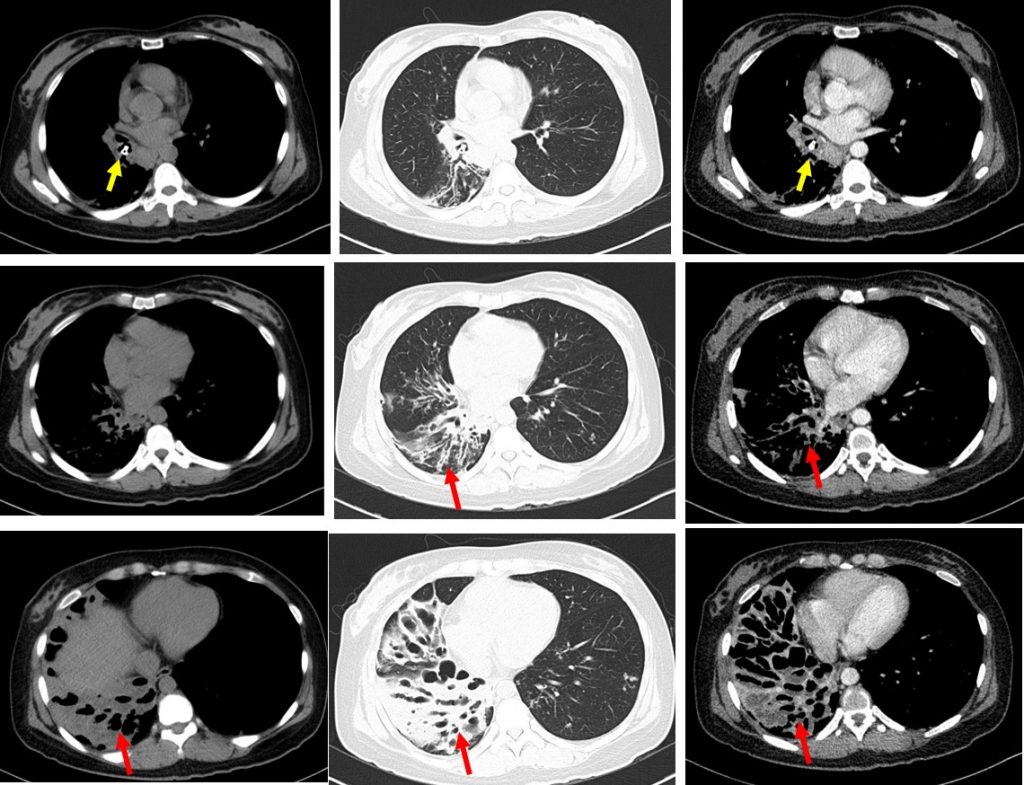
CT scan findings:
- A foreign body of bone density is seen impacted within the right lower lobe bronchus (yellow arrow).
- The adjacent bronchial wall appears irregular and thickened
- Distal to this, multiple saccular dilatation of the distal bronchus in the right lower and middle lobes giving rise to ‘bunch of grapes’ appearance is noted (red arrows).
- Most of the dilated bronchi demonstrate air fluid level within.
- Areas of consolidations and septal thickenings are also seen within the affected lobes.
Diagnosis: Bronchiectasis secondary to foreign body aspiration
Progress of patient:
- Rigid bronchoscopy done.
- Foreign body at right bronchus intermedius and removed
- A calcified chicken bone
- Bronchial alveolar lavage negative for TB, culture and sensitivity also negative, no fungal isolated
Discussion:
- Bronchiectasis is defined by permanent and abnormal widening of the bronchi. It occurs due to chronic airway infection and inflammation
- There are a variety of pathogens involved in bronchiectasis but a common finding is despite the presence of purulent sputum no pathogenic microorganism can be identified.
- The main clinical manifestation is a chronic cough.
- The diagnostic features on imaging include 1) internal diameter of a bronchus is wider than its adjacent pulmonary artery, 2)failure of the bronchi to taper, 3) visualization of bronchi in the outer 1-2 cm of the lung fields
- The main category of bronchiectasis include 1) tubular with smooth dilatation of the bronchi 2) varicose in which the bronchi are dilated with multiple indentations and 3) cystic in which dilated bronchi terminate in blind-ending sacs
- The distribution of bronchiectasis is associated with its different pathophysiologic processes. Most commonly it is generalized and involving the lower lobes.
- Risk factors associated with bronchiectasis include post-infective, mucociliary disorder, obstructive, immune disorder, rheumatic or inflammatory diseases, extremes of age, malnutrition, chronic obstructive pulmonary disease, aspiration, and miscellaneous
- Aspiration of FB into the trachea and subsequently the bronchus can occur in all age groups but more often in infants and little children.
- Early identification and management is important to avoid complications. The incidence of bronchiectasis due to foreign body aspiration is between 1-6% of cases. The risk of bronchiectasis depends on the size, shape, localization and retention of the FB.
- The type of FB and the time of retention are the most common important factors.
Recent Comments