
Case contribution: Dr Radhiana Hassan
Clinical:
- A 30 years old man
- No known medical illness
- Presented with headache, persistent vomiting, reduced hearing over left ear and blurring of vision.
- Clinical examination shows left sensorineural hearing loss with Grade 1 left facial nerve palsy. No limb weakness.
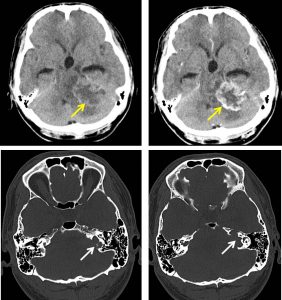
CT scan findings:
- There is a heterogeneous well -defined mass at the left CPA region (yellow arrows)
- It measures about 4.5 cm (AP) x 3.4 (W) x 3.8 cm (CC).
- This mass demonstrated vivid peripheral irregular enhancements post contrast administration. Hypodense centre are observed within, suggestive of necrosis.
- No internal calcification or intra-tumoral haemorrhage.
- Erosion of the left internal auditory canal presents (white arrows) however the semicircular canal and vestibules are intact.
- Mass effect onto the 4th ventricle, pons, and midbrain observed.
- There is hydrocephalus.
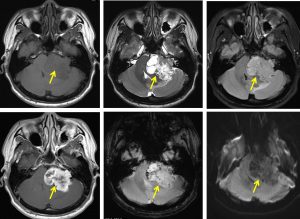
MRI findings:
- There is a large extra-axial, heterogeneous mass with complex cystic and soft tissue component at the left cerebellopontine angle(yellow arrows)
- There is extension into the left internal auditory canal (IAC)
- The lesion exihibit low signal intensity compare to adjacent brain parenchyma on T1 and higher signal on T2. It also shows marked enhancement on post contrast study.
- No areas of restricted diffusion observed on DWI. Blooming artefact are present on GRE.
- The vestibule and semicircular canal appears intact.
- Medially the lesion compressed and displaced the adjacent left cerebellar hemisphere, pons, medulla and 4th ventricle.
- Surrounding perilesional odema observed.
- The supratentorial ventricles are dilated in keeping with obstructive hydrocephalus.
Intraoperative findings:
- Pale greyish highly vascularised tumour. Tumour was debulked centrally and laterally. The anteromedial portion was left behind as it adhered strongly to cerebellar and bleeding upon contact.
- Cranial nerve X1 and XII were identified but Cranial nerve VII was not identified.
HPE findings:
- Macroscopy: specimen labelled as brain tumour consists of multiple pieces of whitish tissue.
- Microscopy: sections show multiple fragments of tumour tissue composed of proliferation of spindle shaped cells arranges as hypercellular area, Antoni A and hypocellular area, Antoni B. The hypercellular area displays palisading of nuclei forming verocay bodies. There is no increase in mitosis or necrosis seen. Hyalinization of blood vessels is present in areas.
- Immunohistochemistry: the spindle cells are diffusely positive for S100 antibody.
- Interpretation: Schwannoma
Diagnosis: CPA schwannoma
Progress of patient:
- Insertion of right ventriculoperioneal shunt for hydrocephalus was done
- Subsequently patient had left retrosigmoid craniectomy and tumour debulking
- Post surgery patient recovered well with no facial nerve palsy.
- Patient was subsequently referred to other hospital for further treatment
Discussion:
- Schwannomas are benign tumours of schwann cell origin.
- Almost all intracranial schwannomas are related to cranial nerves.
- Majority are solitary (90%) and located at CP angle region.
- It causes enlargement of IAC (>2mm difference between right and left IAC or IAC> 8mm)
- Can be isodense on CT scan with dense enhancement post contrast. It may contain cystic degenerative areas.
Recent Comments