
Case contribution: Dr Radhiana Hassan
Clinical:
- A 65 years old man with underlying DM
- Presented with abnormal movement at left upper limb for 5 days
- Become more prominent day by day
- Unable to control the movement
- Interfere with daily activity
- Clincal examination shows left hemibalism involving the left upper and lower limb
- No parkinsonism or dystonia, no ataxic gait
- Power 5/5
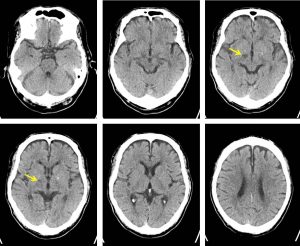
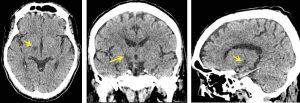
CT scan findings:
- There is a well-defined hypodensity in the right subthalamic region
- No mass effect or surrounding oedema
- No effacement of adjacent sulci
- No other abnormality seen
Diagnosis: Subthalamic infarction
Discussion:
- Hemiballismus consists of intermittent, large-scale flinging movement of one side of the body. It resemble chorea except that they are unilateral, less predictable and more forceful.
- Classic imaging findings associated with hemiballismus is contralateral subthalamic nucleus abnormality. However lesions are found in less than one third of cases.
- Alternatively lesions in the caudate nucleus or basal ganglia may be responsible.
- Patient with hemiballlismus do not have cormorbid congnitive impairment, seizures or paresis.
- The majority of hemiballismus are due to a vascular event, hyperglycaemia or opportunistic infection in an immunocompromised patient, and therefore the history and examination should be directed toward these aetiologies.
- MRI is preferable for most conditions, but may require sedation or anesthesia in order to allow the patient to be scanned. For patients with recent onset of hemiballismus, urgent hospitalization is reasonable.
- The subthalamic nuclei are small paired structures that are part of the functional basal ganglia located ventral to the thalamus, dorsal to the substantia nigra and medial to the internal capsule.
- Although hemiballismus is disabling, it is usually self-limiting and lasts for 6-8 weeks.
- Treatment with antipsychotic is usually effective. It is important to treat any underlying causes.
Recent Comments