
Case contribution: Dr Radhiana Hassan
Clinical:
- A 25 years old student
- Presented with fever and left loin pain for 3 weeks
- Clinical examination shows ballotable mass at left loin
- Ultrasound shows mass lesion at left kidney
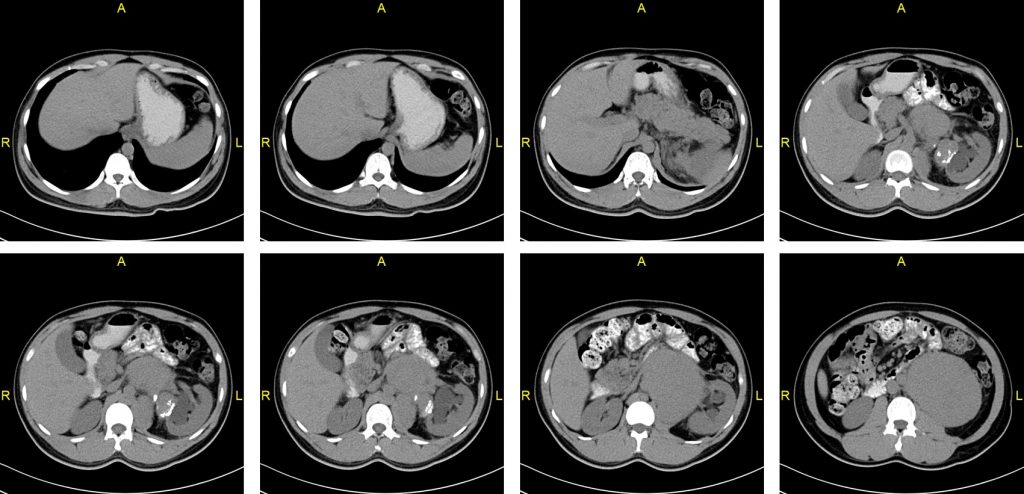
CT scan findings:
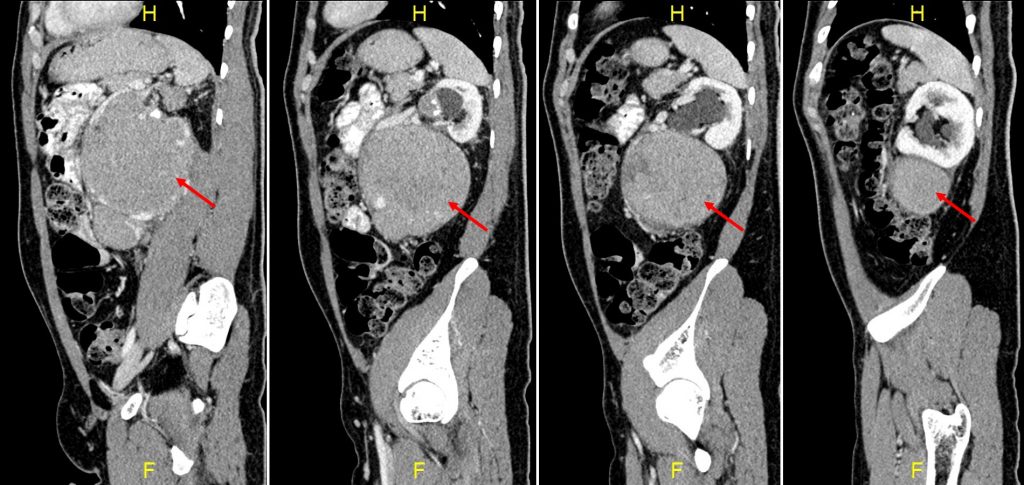
- Images in axial soft tissue window plain and contrast-enhanced, sagittal contrast-enhanced soft tissue window
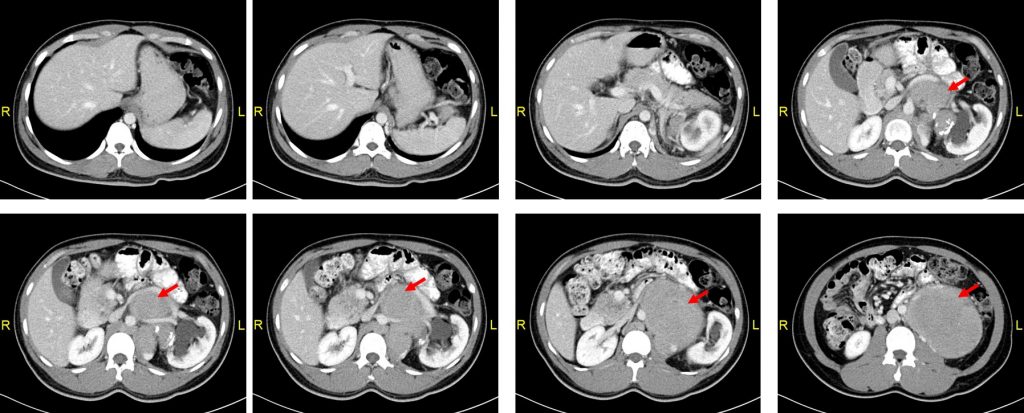
- A large lobulated oval shaped mass is seen at the left retroperitoneal region measuring 13 cm in its largest dimension
- This mass is heterogeneously enhancing in post contrast study. Hypodense areas are seen at the periphery of the mass suggestive of necrotic/cystic component. Multiple dilated vessels are seen insinuating in between the mass.
- Superiorly the mass extends until the pancreas just inferior to the splenic vein. Medially the mass has poor demarcation with the abdominal aorta from the level of L1 to L3 vertebral bodies. However both vessels are still patent. Inferiorly the mass ends at the level of L4/L5 intervertebral disc. Clear demarcation is observed between the mass and the left psoas muscle.
- The mass appears to encase the left renal artery and displaced as well as stretch the left renal vein superoanteriorly.
- The mass is compressing on the left pelvi-ureteric junction causing left moderate hydronephrosis. It pushes the left kidney laterally, abdominal aorta and the left psoas muscles medially. The mass also seen to push the D3/D4 part of the duodenum and proximal jejunum superoanteriorly.
- There is a calcified hypodense lesion abutting medial part of upper pole of the left kidney measuring about 2.2 x 4.2 cm . This could represent calcified lymph nodes. Multiple matted paraaortic lymph nodes are also seen with the largest measuring about 1.8 cm.
HPE result and Diagnosis:
- Left retroperitoneal neuroendocrine tumour grade 1
Discussion:
- Neuroendocrine tumours (NRTs) represent wide spectrum of diseases. It ranges from carcinoid tumour, pheochromocytoma, GI NETs, pancreatic NET, pulmonary NETs, thyroid medullary tumours and Merkel cell carcinoma. Gastroenteropancreatic NETs are the largest group of primary NETs that arise in the abdominal cavity.
- It can also be divided as functioning or non-functioning, slow-growing and more aggressive lesions and so on.
- Primary neuroendocrine tumours of the retroperitoneum are extremely rare. NETs found in the retroperitoneum are usually metastatic.
- Retroperitoneal NETs are more commonly seen in 4th-6th decades with a median age of 54 years old
- A slight female predominance noted
- Most retroperitoneal NETs are asymptomatic or presented with non-specific symptoms. No carcinoid syndrome associated with this tumour (non-functioning tumour)
- Most retroperitoneal NETs are large in size at presentation ranges from 4-21 cm.
- On imaging it is seen as well-defined, hypervascular mass round or ovoid homogenous solid lesion. Large tumours may have cystic component, hemorrhage and necrotic areas. No calcification within the mass. Enhancement can be homogenous, ring-like or heterogenous.
- Differential diagnosis include plexiform neurofibroma, lymphangiomyomatosis, primary retroperitoneal mucinous cystadenocarcinoma
Recent Comments