
Case Contribution: Dr Radhiana Hassan
Clinical:
- A 43 year old male with no known medical illness.
- Referred from district hospital with initial CT brain shows pineal region mass with hydrocephalus.
- Presented with progressively worsening headache for 2 months associated with worsening vision and multiple fall due to giddiness.
- On examination, GCS E4V5M6, pupil was reactive and symmetrical. He had no opthalmoplegia. No motor deficit. Cerebellar sign was negative.
- Right burr hole, endoscopic examination with VP shunt was performed.
- He was extubated post VP shunt and re-admitted for MRI Brain.
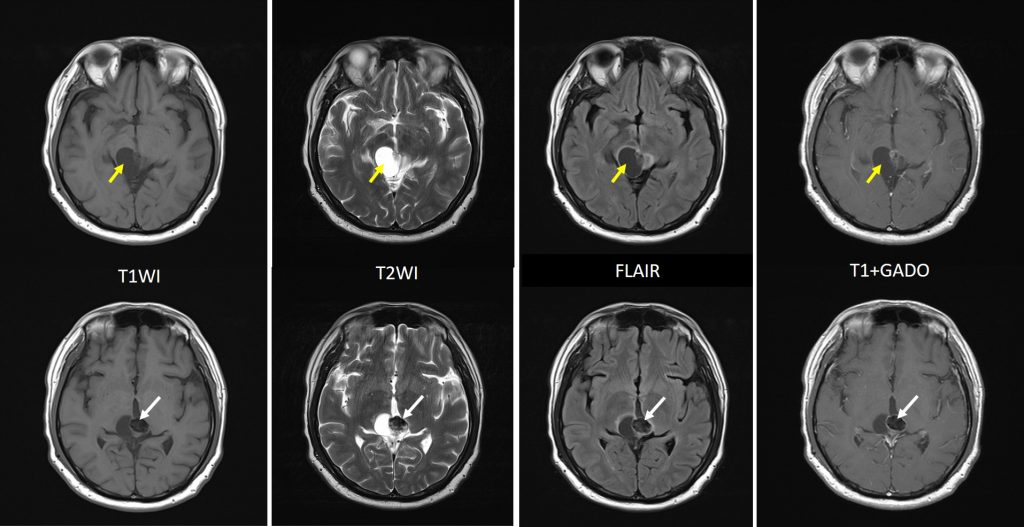
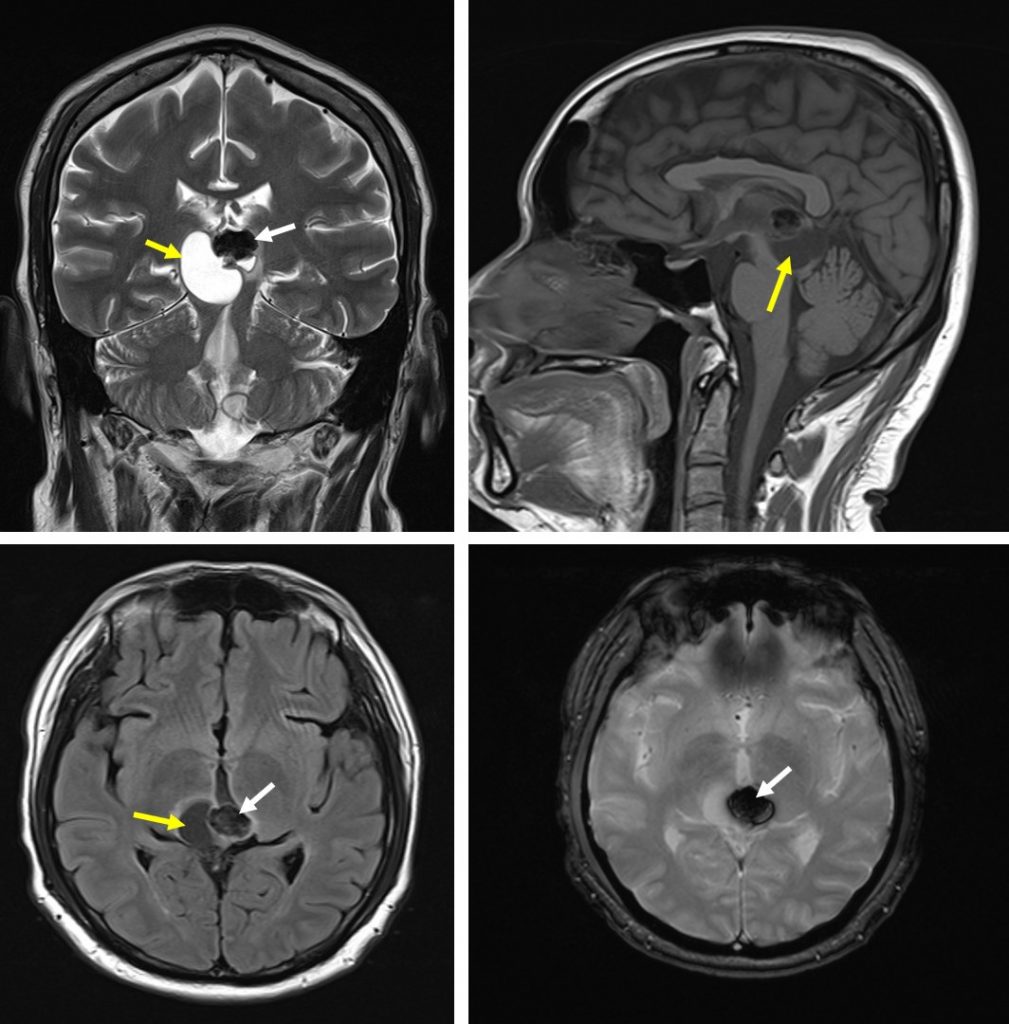
MRI findings:
- A well-circumscribed lesion at the pineal region, mainly hypointense on T1, hyperintense on T2 and not enhanced post contrast suggestive of cystic lesion.
- An oval lesion periphery to this cystic lesion is seen which is hypointense on all sequence and shows blooming artifact on GRE sequence suggestive of a calcification.
- A small area suggestive of soft tissue component with enhancement is seen below the area of calcification.
- Compression to the tectal plate and thalamus on the right side
- Minimal perilesional oedema
Progress of patient:
- Underwent sub occipital craniotomy and tumor excision.
- He was extubated post op day 1 and discharged well after 4 days with review HPE in subsequent clinic follow up.
- HPE: Pineal parenchymal tumor of intermediate differentiation (PPTID).
- Post op MRI Brain and Spine were done after oncology consultation;
- MRI Brain post operative: residual cystic component of pineal lesion with similar size of solid component and calcification.
- MRI Spine: No MR evidence of drop metastases
- Patient was planned for gamma knife radiosurgery.
Diagnosis: Pineal parenchymal tumor of intermediate differentiation (PPTID).
Discussion:
- Mass at pineal region can cause a defect in up-gaxe (Parinaud syndrome) due to compression of tectal plate.
- It can also cause obstructive hydrocephalus due to compression of cerebral aqueduct.
- Pineal parenchymal tumours are seen in about 30% of primary pineal region tumours.
- Pineal parenchymal tumours of intermediate differentiation (PPTID) are tumours that fall between pineocytoma (WHO Grade 1) and pineoblastoma (WHO grade 4). It is considered as WHO grade 2 or 3 tumours
- The radiographic appearances are also intermediate.
- PPTID is commonly seen in middle-aged adult aged 20-70 years with slight female predilection (similar to pineocytomas)
- Can extend into adjacent structures (ventricles, tectum, thalamus). CSF dissemination is rare
- CT scan seen as hyperdense mass centered in pineal region which engulfs pineal gland calcification. Gross hemorrhage and cysts are rare. Hydrocephalus is common. Post contrast: strong uniform enhancement
- MRI shows a lesion with T1WI-mixed iso and hypointense, T2WI-isointense to gray matter, small cystic appearing foci is common, FLAIR-hyperintense, GRE-foci of blooming, calcification is common, hemorrhage is rare, post contrast shows strong heterogenous enhancement.
- Differential diagnosis: germinoma, pineocytoma, pineoblastoma, papillary tumour of pineal region
- It may invade adjacent structures ad also spread along CSF and therefore imaging of the entire craniospinal axis is required
- Treatment and prognosis fall between pineocytomas and pineoblastomas
Recent Comments